Definition
Esophageal diverticula are sac-like protrusions, similar to sacs or pockets, which form in the wall of the esophagus. The causes that determine their onset include the increase in pressure inside the esophagus, points weakness of its wall, and scarring of the periesophageal tissues (surrounding the esophagus).
The stagnation of bolus inside these sacs (diverticula) can give rise to episodes of regurgitation and be associated with complications such as inflammation and / or perforation of the bowel. Diverticula can form at any level of the esophagus, but mainly involve the distal portion of the cervical and thoracic tracts.
The most frequent diverticular manifestation of the esophagus is Zenker's diverticulum.

Classification
There are several ways to classify esophageal diverticula; first, they can be congenital (present from birth) or acquired (they can develop over the course of life). Congenital esophageal diverticula often result from excessive weakness of the esophageal wall, while acquired forms they are distinguished in drive or traction diverticula.
From the histopathological point of view, we can distinguish:
- true diverticula: they affect all the layers of the esophageal wall (mucosa, submucosa, muscle and adventitia);
- false diverticula, also known as pseudo-diverticula: they originate from the herniation of the mucosa and submucosa when there is a resistance defect in the muscle wall (example: Zenker's diverticulum).
Based on the location, we can instead distinguish:
- hypopharyngeal or cervical or pharyngo-esophageal diverticula (upper third of the esophagus)
- parabronchial or mid-thoracic diverticula (middle III ° tract)
- epiphrenic diverticula (lower III ° tract)
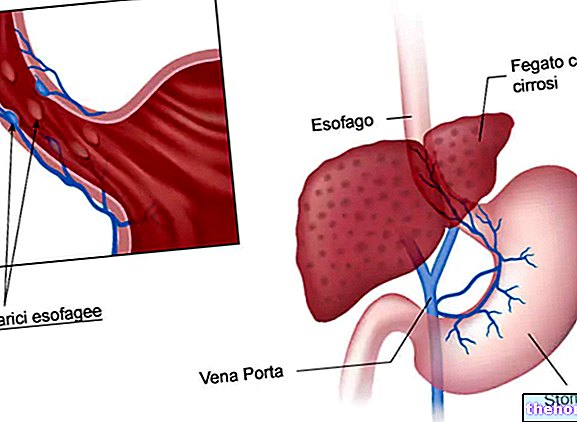
Notes on anatomy: the esophagus
The esophagus is a muscular tube, about 25 cm long, whose primary function is to carry food from the pharynx to the stomach.
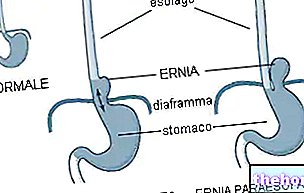
The passage of food from the pharynx to the esophagus is regulated by the upper esophageal sphincter (SES), which acts as a barrier to esophagus-pharyngeal reflux and corresponds to a high pressure zone. The esophagus passes into the mediastinal cavity ( located between the trachea and the vertebral column), before crossing the diaphragm (the large muscle that divides the chest from the abdomen) at the esophageal hiatus. At the lower end of the esophagus there is the sphincter lower esophageal (SEI), a ring of smooth muscle that regulates the passage of food from the esophagus to the stomach, acting as a barrier to gastroesophageal reflux.
Classification
- Diverticula of congenital type: from impaired esophageal development.
- Pseudodiverticula: consequent to the dilation of the glands of the esophageal submucosa. They can occur in single or multiple form. They are also called intramural diverticula, as they are confined to the thickness of the wall.
- Diverticula proper: by drive or by traction.
- Drive diverticula: these are mucosal hernias, which extend through the muscular layers of the esophagus. They are formed as a result of increased intraluminal pressure, associated with abnormal regional peristalsis. They are typically pharyngo-esophageal (example: Zenker's diverticulum, which in any case is a false diverticulum) and epiphrenic (caused by dyskinesias such as "achalasia," an alteration that causes the progressive loss of esophageal peristalsis).
- Traction diverticula: they extend to the entire thickness of the esophageal wall. They are mostly mid-thoracic and can be of congenital origin or secondary to fibrous adhesions (scars) produced as a result of an inflammatory disease (bronchopneumonia or pulmonary inflammatory processes) that has affected the organs close to the esophagus (especially lymph nodes) .
Epidemiology
Most esophageal diverticula begin in middle-aged and older adults. The presentation of the pathology in infants and children occurs rarely.
In particular, Zenker's diverticula are typically found in people over the age of fifty.
Cause and effect
Esophageal diverticula can mainly form according to the following mechanisms:
- structural lesions or impaired motility of the esophagus: usually derive from a weakening of the muscular seal of the esophageal mucosa and are caused by motor abnormalities.
In fact, the structure and motility of the esophagus may not be compliant for:
- relaxation of muscle tissue;
- lack of coordination at the level of the lower esophageal sphincter;
- the presence of stenosis (narrowing of the lumen).
The lining of the esophagus, under the pressure of the internal pressure of the organ, can protrude through a weak point of its muscular wall, as in the case of Zenker's diverticulum.
- adhesions or inflammatory processes: the origin in traction diverticula, usually middle-esophageal or epiphrenic, is due to the presence of extraluminal extrinsic adhesions, which can cause the esophageal wall to protrude.
In the early stages, the presence of protrusions in the wall of the esophagus causes only some swallowing disturbances: the food swallowed tends to stop at the level of the diverticulum and the patient has the sensation that a foreign body is present in the throat.
As the disorder progresses, the disease can increase in size, affecting breathing (it can compress the trachea and cause breathing difficulties).
Finally, serious complications can also arise: in addition to regurgitation, food that becomes blocked at the level of the diverticulum can stagnate and infect the wall of the esophagus, causing perforation of the sac and spreading the infection to nearby tissues.
Symptoms
For further information: Symptoms Esophageal diverticula
Often patients affected by the disease are asymptomatic. In other cases, the presence of esophageal diverticula can cause:
- dysphagia (difficulty in swallowing, feeling of obstruction);
- food obstruction (choking);
- symptoms of varying severity related to esophageal dyskinesias;
- food regurgitation: reappearance of ingested food;
- chest pain;
- cough (some foods may be regurgitated into the airways);
- dyspnoea: difficulty in breathing or shortness of breath;
- halitosis: it can be present as a secondary consequence of food residues that become blocked at the level of the lesion;
- gurgling noises when swallowing;
- potential infection of the pharyngeal areas due to the food introduced that accumulate at the level of the diverticulum.
In rare cases, perforation or bleeding of the esophageal diverticulum may occur.
In the event that a Zenker's diverticulum reaches a large size, a palpable swelling on the neck may occur.
Complications
- Chronic esophagitis;
- Inflammation;
- Inhalation pneumonia;
- Perforation, resulting in mediastinitis or esophagus-tracheo-bronchial fistula formation;
- Hemorrhage;
- Carcinoma.
Esophageal diverticula: diagnosis and therapy "






-feofitina-di-rame---e141-(ii)-sali-di-sodio-o-potassio-dei-complessi-della-clorofilla-con-rame.jpg)