Generality
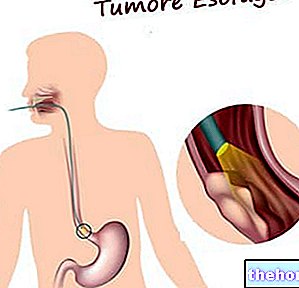
Esophageal cancer is a neoplastic process that originates from the tissues of the esophagus (the channel through which ingested food and liquids reach the stomach).

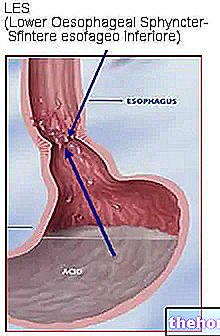
The main factors predisposing to the onset of esophageal cancer are chronic alcohol ingestion, tobacco use, achalasia, gastroesophageal acid reflux and / or Barrett's esophagus.
At the onset, esophageal cancer manifests itself with swallowing problems: usually, the difficulties appear gradually, first for solid foods and then for liquid ones. Other symptoms are progressive weight loss, reflux, chest pain and hoarseness Over time, esophageal cancer can grow, invade neighboring tissues, and also spread to other parts of the body.
Diagnosis is established with endoscopy, followed by computed tomography (CT) and endoscopic ultrasound for staging.
Treatment varies according to the stage of the esophageal cancer and generally consists of surgery, in combination or not with chemotherapy and / or radiotherapy. Long-term survival is poor, except in cases with localized disease.
Notes on anatomy
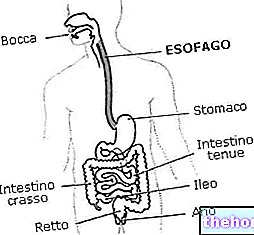
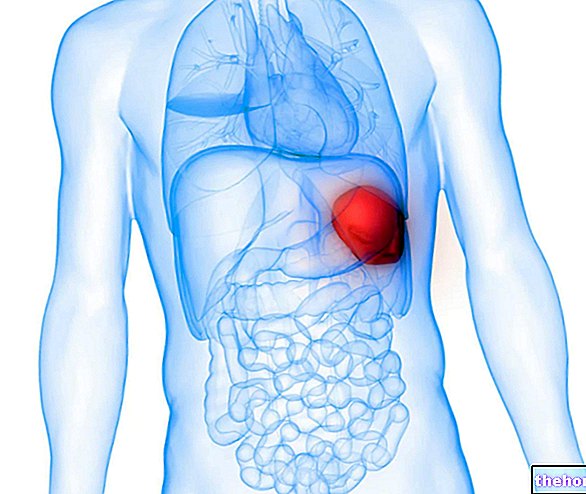
- The esophagus is a muscle-membranous duct, about 25-30 centimeters long and 2-3 cm wide, which connects the pharynx to the stomach. This structure is located almost entirely in the chest, in front of the vertebral column.
- The walls of the esophagus are made up of a layer of epithelial lining similar to that of the mouth, while they are externally surrounded by two layers of smooth muscle.
- By contracting in the act of swallowing, the muscular component pushes the food downwards, towards the stomach, from which the esodagus is separated by a valve, called cardia, which prevents ingested food and gastric juices from rising.
- The mucosa of the esophagus is rich in mucus-producing glands, which have the function of lubricating the walls, facilitating the transit of swallowed food.
Causes and risk factors
Esophageal cancer is caused by the uncontrolled growth and proliferation of some cells that make up the organ, induced by an alteration in their DNA. The reasons for the origin of this event are not yet completely clear, but it seems that the neoplastic process may depend on the combination of genetic factors, diet, lifestyle and previous esophageal pathology (such as reflux esophagitis, caustic strictures and Barrett's esophagus). The common pathogenesis of these conditions would be the presence of a chronic inflammatory state of the esophageal mucosa which, through the various degrees of dysplasia, would lead to neoplasia over time.
The main factors that can contribute to esophageal cancer are:
- Alcoholism;
- Use of tobacco (smoked or chewed);
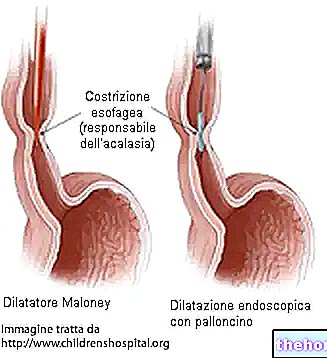
- Esophageal achalasia (pathological condition that affects the muscles of the esophagus and makes swallowing difficult);
- Chronic inflammation, including peptic esophagitis, gastroesophageal reflux and / or Barrett's esophagus;
- Ingestion of hot food and drinks;
- Diet low in fresh fruit and vegetables;
- Increased intake of red meats;
- Obesity.
Other conditions that can favor esophageal cancer are:
- Human papillomavirus infections;
- Palmar and plantar tylosis (rare hereditary disease characterized by thickening of the skin on the palms of the hands and soles of the feet);
- Caustic injuries;
- Previous radiant therapies;
- Plummer-Vinson syndrome (condition characterized by the clinical triad of dysphagia, iron deficiency anemia and membranes in the esophageal lumen).
Other risk factors for esophageal cancer are:
- Age: the incidence progressively increases after 45-50 years; most cases are found between 55 and 70 years;
- Gender: men are more affected than women, with a ratio of 3 to 1.
Main types
Depending on the tissue from which it originates, two main forms of esophageal cancer are distinguished:
- Squamous cell carcinoma (or squamous cell): it is the most common of esophageal tumors (it represents about 60% of cases): it originates from the squamous cells that cover the internal wall of the organ.
It usually develops in the upper and middle portions, but can occur along the entire esophageal canal. - Adenocarcinoma: it constitutes about 30% of the tumors of the esophagus and derives from the transformation in a neoplastic sense of the gland cells responsible for the production of mucus. The adenocarcinoma occurs more frequently in the last section of the esophageal canal, near the junction with the stomach ( lower third). This neoplasm can also originate from islands of gastric mucosa out of the site or from glands of the cardia or submucosa of the esophagus.
Less common malignant esophageal tumors include sarcoma, primary small cell carcinoma, carcinoid, and primary malignant melanoma.
In about 3% of cases, esophageal cancer can originate from the metastasis of other neoplasms (especially melanoma and breast cancer). These processes usually involve the loose connective tissue around the esophagus, while primary carcinomas originate in the mucosa or submucosa.
Signs and symptoms
For further information: Symptoms Tumor of the "esophagus"
In the early stages, esophageal cancer tends to be asymptomatic.
The most frequent onset symptom is difficulty in ingesting food (dysphagia), which generally coincides with the narrowing of the lumen of the esophagus.
At the beginning, the patient experiences a difficulty in swallowing or a sensation that solid foods stop during their passage to the stomach; this manifestation from episodic becomes constant and then extends to semi-solid foods and, finally, to liquids and saliva. This constant progression suggests an expansive malignant process rather than esophageal spasm or peptic stenosis. In more advanced stages of tumor development, swallowing can also become painful (odynophagia). When the tumor mass hinders descent of food along the esophagus, episodes of regurgitation may occur.
Weight loss is inexplicable and almost constant, even when the patient retains a good appetite.
Growth of the tumor out of the esophagus can cause:
- Paralysis of the vocal cords, hoarseness and / or dysphonia (the alteration of the tone of voice is secondary to the compression of the recurrent laryngeal nerve, which innervates all the intrinsic muscles of the larynx);
- Hiccups or paralysis of the diaphragm
- Chest pain, often radiating to the back.
Intraluminal involvement of the neoplastic mass can cause:
- Painful cramps of the esophagus;
- Heartburn or frequent belching (reflux);
- He retched;
- Iron deficiency anemia;
- Expulsion of blood with vomiting (haematemesis);
- Picee stool evacuation (melena);
- Inhalation cough and bronchopneumonia.
In more advanced forms, fluid may also form in the lining of the lung (pleural effusion), with the onset of dyspnea (difficulty in breathing). Other manifestations may include: increased liver size and bone pain, usually associated with the presence of metastases.
The esophagus is drained along its entire length by a lymphatic plexus, so lymphatic diffusion through the lymph node chains on the sides of the neck and above the collarbone is common, with appreciable swelling at these levels.
Esophageal cancer usually metastasizes to the lungs and liver and sometimes to distant sites (e.g., bones, heart, brain, adrenal glands, kidneys, and peritoneum).
Diagnosis
The diagnosis of esophageal cancer is made with endoscopy of the esophagus (esophagoscopy), associated with biopsy and cytology.
During this investigation, a flexible, thin and illuminated instrument (called an endoscope) is introduced from the mouth to allow the doctor to directly observe the morphological structure of the esophagus and stomach.

In addition, it is possible that the patient undergoes an x-ray of the esophagus with contrast medium. barium, capable of making any obstructive lesion more evident and excluding the presence of associated diseases.
The association of the two procedures (esophagoscopy and radiography) increases the diagnostic sensitivity up to 99%.