Outline of anatomy and physiology
The esophagus is a hollow tube-shaped organ (25-30 cm long) that connects the pharynx to the stomach; the esophagus is limited above by the upper esophageal sphincter (or cricopharyngeal) and below by the lower esophageal sphincter (or cardia).

From the histological point of view, the esophagus is made up of 4-5 layers; proceeding from the inside (lumen) towards the outside, in order they are: mucosa, submucosa, muscle, adventitia and serous (present only in the portion closest to the stomach).
NB. The esophagus is an organ involved in swallowing, a process useful for transporting the food bolus from the mouth to the stomach; this movement begins voluntarily (tongue, glottis, etc.) and then changes into an involuntary movement. This means that the upper portion of the " esophagus possesses a striated musculature that contracts by the will of the subject (such as that of the musculoskeletal system to be clear), while the lower esophageal tract is characterized by smooth muscles (such as that of the stomach and intestine), therefore involuntary.
Insights: the mechanism of DEGLUTITION
Swallowing is based on the synchrony and coordination between the larynx, pharynx and esophagus, and takes place in 3 distinct phases:
- Oral phase, voluntary, the bolus is pushed by the tongue into the back of the mouth.
- Pharyngeal phase, involuntary and reflex, consists in the passage of food in the esophagus through the pharynx; in this phase the epiglottis is displaced posteriorly and prevents the passage of the bolus in the respiratory tract.
- Esophageal phase, involuntary, favors the transit of the bolus to the stomach thanks to the esophageal peristalsis ("wave" movement that squeezes the "esophagus from top to bottom). There are two types of esophageal peristalsis: primary or triggered by swallowing and secondary or generated by esophageal distension).
Illnesses
It is possible to affirm that the diseases of the esophagus are secondary to an "impaired motility of the whole organ. Specifically, diseases of the esophagus can be classified into:
- Hypermotility diseases, ie caused by an "increased contractile capacity" of the esophagus
- Hypomotility diseases, that is determined by a lower contractile capacity of the esophagus.
Hypermotility diseases
These disorders are characterized by: the presence of violent and / or uncoordinated muscular contractions of the food bolus advancement (peristaltic waves), and the inability to release the esophageal sphincter.
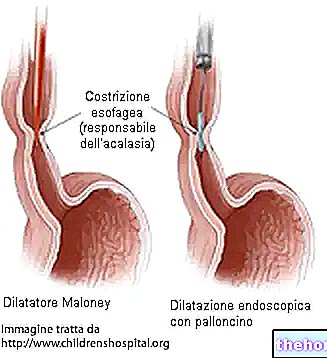
Achalasia: disease that concerns the failure to release the lower esophageal sphincter associated with an absent or incoordinated movement of the "esophagus. It is frequently caused by the depletion of neurons that inhibit muscle tone and the most indicative symptom is Dysphagia, or the sensation of bolus arrest. "behind the breastbone". It is a kind of so-called dysphagia paradox as it involves both the ingestion of liquids and solids, and therefore differs from progressive dysphagia which mainly concerns liquids; it is frequently accompanied by the regurgitation of food material. The diagnosis is made through manometry which measures both the absence of esophageal muscle movement and the increase in pressure of the lower esophageal sphincter. The therapies are different: pharmacological (by injection), endoscopic dilation of the sphincter and surgical.
Nutcracker esophagus and corkscrew esophagus: Nutcracker esophagus disease causes contractions normally coordinated but with average amplitude and duration exceeding the norm, which are felt in a highly painful way. The corkscrew esophagus (or diffuse esophageal spasm) is characterized by numerous uncoordinated contractions not peristaltic ( simultaneous, therefore non-propulsive), which occur after swallowing with anginal-like pain. These are diseases of the esophagus associated with psycho-physical stress conditions, which can be diagnosed by means of a manometric examination and can be treated pharmacologically.
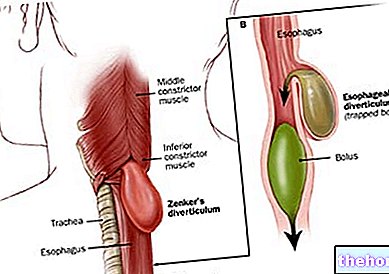
Esophageal diverticula: they can be genetic or acquired. Those acquired can be caused by a gradual extroversion of the mucosa and submucosa as an effect of an "increased pressure (called acquired) or by scar retraction on the wall of the" esophagus (called "traction").
Hypo-mobility disorders
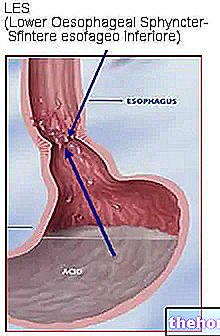
They are diseases of the esophagus characterized by the constricting ineffectiveness of the lower esophageal sphincter; the main clinical manifestation is gastroesophageal reflux (GERD).
Gastro-oesophageal reflux disease (GERD): generally asymptomatic esophageal disease which in the long term can compromise the integrity of the mucosa; GERD determines: burning (heartburn) localized in the retrosternal area (due to the acid action of the gastric contents on the mucous membrane of the esophagus), the regurgitation of acidic material and epigastric pain (felt just below the sternum). The tests to diagnose GERD are mainly esophagogastroduodenoscopy and 24-hour PHmetria. The treatment consists mainly of drug therapy and diet therapy.
If neglected, GERD can become complicated and result in esophagitis or, worse, Barrett's esophagus.
NB. It was decided NOT to deal with the "topic" tumors of the "esophagus" as it is already fully described together with the relative chapter entitled "Drugs to treat" esophageal cancer "which can be found on our website.
CONTINUE: Nutrition for diseases of the "esophagus"
Bibliography:
- Gastrenterology manual for dieticians - National Coordination of University Teachers of Gastroenterology - Italian Gastroenterological Publishing - page 48:50