Generality
We speak of Barrett's esophagus when the normal tissue that lines this muscular duct, located between the pharynx and the pit of the stomach, is replaced with an epithelium similar to the one that internally covers the walls of the duodenum (initial section of the small intestine).

Causes
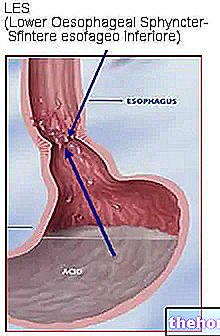
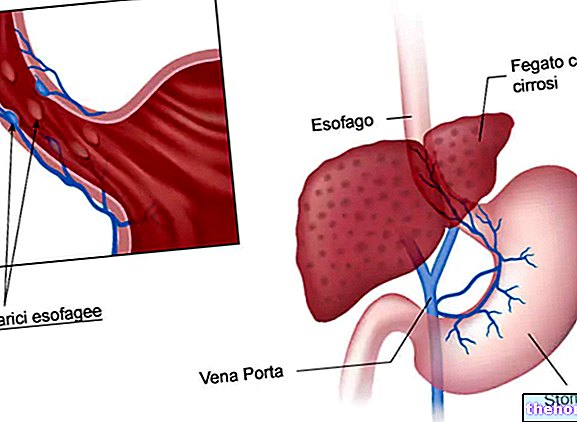
Barrett's esophagus is a typical complication of gastroesophageal reflux. Following the relaxation of the sphincter that virtually separates the esophagus from the stomach (called cardia), the ascent of gastric juice into the esophagus determines - in the long run - a modification of the epithelium. esophageal, which thus tries to defend itself from the acid. Epithelial cells therefore take on characteristics very similar to gastric or duodenal cells, characterizing the condition known as Barrett's esophagus. This complication is considered pre-cancerous, since the abnormal epithelium can undergo uncontrolled replication (cancer).

Data in hand, Barrett's esophagus is found in 15-20% of patients with chronic gastroesophageal reflux disease (GERD), mainly in Caucasian men aged 50 or over.
According to recent epidemiological studies, the risk of developing adenocarcinoma in the presence of Barrett's esophagus is estimated at 0.4 - 0.5% per year per patient, while the 5-year survival rate from the diagnosis of adenocarcinoma (esophageal cancer) is very low (less than 10%). In the light of these data, even if the risk is all in all modest, it is desirable to perform an endoscopic examination in all patients suffering from reflux, in order to exclude with certainty the presence of Barrett's esophagus.
POTENTIAL RISK FACTORS
- gastroesophageal reflux disease,
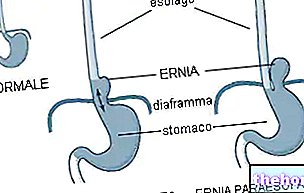
- hiatal hernia,
- overweight, c
- alcohol consumption,
- smoke,
- male sex (men are twice as at risk as women),
- Ethnicity: Caucasian,
- old age,
- family members with Barrett's esophagus.
Symptoms
For further information: Barrett's Esophagus Symptoms
Barrett's esophagus is an asymptomatic condition in itself, which, however, is frequently accompanied by the typical symptoms of the reflux disease that generated it (acid regurgitation, heartburn, difficulty in swallowing food and back pain; in the most severe cases they can be note blackish and tarry stools, and traces of blood in the vomit).
The severity of Barrett's esophagus depends not so much on the symptoms and related disorders, but on its potential evolution to adenocarcinoma (esophageal cancer).
Diagnosis
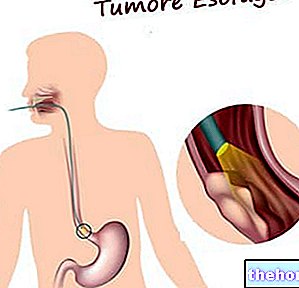
As anticipated, the diagnosis of Barrett's esophagus is based on the results of endoscopy and esophageal biopsy. A thin tube (endoscope), equipped with a light source and a camera at the end, is made to go down the patient's throat, examining the state of health of the esophageal epithelium and looking for any metaplasias. In the event that these are present, using special instruments slid along the endoscope, the doctor takes small samples of abnormal tissue, which are subsequently examined microscopically by the "expert anatomopathologist. The report will therefore be able to speak or not of dysplasia on metaplasic tissue and establish its severity (low grade or high grade) based on the structural differences with the typical cells of the esophagus." The greater the dysplastic degree, the greater the risk of tumor evolution; for example, if the dysplasia is particularly severe, the risk can rise up to 10% or more per patient year. Remember, however, that the dysplastic process is not a tumor process and can be reversible (while a transformed tumor cell can no longer return to normal).
Gastroesophageal reflux → esophagitis → Barrett's esophagus, metaplasia → dysplasia → adenocarcinoma
Metaplasia is basically the transformation of a cell of one type (eg esophageal) into a cell of another type (eg intestinal).
Dysplasia is the abnormal proliferation of a group of cells that have lost the typical characteristics of the tissue to which they belong, returning to the most primitive form and rapidly reproducing; it is a localized proliferation which, especially when of a high degree, can evolve into carcinoma in situ.
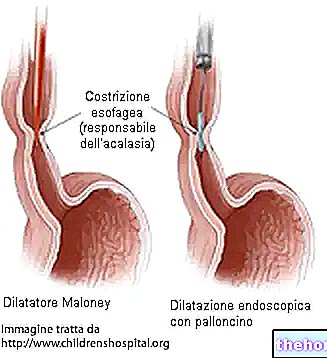
Treatment
Barrett's esophagus therapy must aim both at controlling the symptoms of gastroesophageal reflux and at healing esophagitis, but above all it must aim at restoring the normal esophageal squamous epithelium in areas of previous intestinal metaplasia. In this regard, the so-called proton pump inhibitors are used, drugs capable of significantly reducing gastric acidity for a long time (18-24 hours). Although these drugs are very effective in eliminating the acid insult and reducing symptoms associated with reflux disease, in many cases fail to produce significant regression of the dysplastic tissue.
In the event that Barrett's esophagus is characterized by a low degree of dysplasia, the situation is periodically monitored through endoscopic examinations every 12-36 months. Conversely, in the event that a high degree dysplasia is present, it may be necessary to remove o destroy the abnormal tissue (through special endoscopic instruments or with ablation by radiofrequency or laser); much more rarely the entire portion affected by Barrett's esophagus is exported and in this case the residual tract is stitched up with the pit of the stomach.
Other articles on "Barrett's Esophagus"
- Medicines for the treatment of esophagitis
- Esophagitis
- Esophagitis: diagnosis and treatment
- Medicines for the treatment of Barret's esophagus
- Diet for esophagitis