Diseases affecting the esophagus cause impaired swallowing, delivery of the bolus in the stomach and gastric containment.
Generally speaking, nutrition is NOT directly involved in the pathogenesis of these diseases, however it can be decisive in reducing symptoms and related complications, both in the short and long term.
Esophagus and diseases
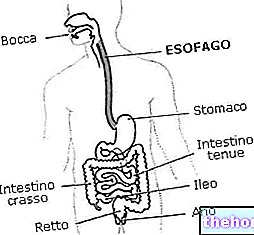
The esophagus is an organ that connects the mouth and the stomach; it is hollow, tubular in shape and about 25-30 cm long in the adult. The esophagus starts from the cricopharyngeal sphincter (above) and ends with the cardia (below).
Like all anatomical structures of the human body, the "esophagus is subject to pathological alterations that compromise its structural integrity, consequently the physiological mechanism of action. It is therefore possible to deduce that diseases of the esophagus essentially determine the"impaired peristaltic motility ... which translated in layman's terms means the impaired food transport from the pharynx to the stomach. This occurs thanks to a "wave" movement that progressively squeezes the esophageal contents from top to bottom: while a segment of upstream esophageal musculature contracts, the downstream stretch relaxes; subsequently it will be the latter to contract and so away, in succession from top to bottom until the complete descent of the food bolus into the stomach.
Diseases of the esophagus are of two types: some called da hypermotility, that is determined by: an "increased contractile capacity in concomitance with a lack of coordination between stimuli and the inability to release the cardia; others classifiable by hypomotility, or generated by the insufficient containment of the cardia. Regarding the latter, the predominant clinical manifestation is GERD - gastroesophageal reflux disease which, if neglected, can lead to chronic inflammation up to determining esophagitis and / or esophagus of Barrett.
Nutrition in reflux disease
The hygienic-alimentary advice concerning diseases of the esophagus, in reality, basically refers to gastroesophageal reflux disease (GERD).
GERD is a chronic and potentially relapsing disease, therefore "specific nutrition" should not be considered a transient therapy, but a lifelong condition.

Gastro-esophageal reflux disease is frequently associated with another disorder, or rather, with an "anatomical alteration that tends to worsen the symptoms and related complications: l "hiatal hernia; the latter is nothing more than an invagination (a kind of "sucking") of the upper gastric portion (heart part) above the diaphragm, where the esophagus should end.
Hiatal hernia, GERD and related complications are closely related to inappropriate eating habits, overweight and especially visceral obesity; it follows that, in the event that the subjects suffering from GERD and hiatal hernia are characterized by an excess of fat or visceral fat, the first dietary measure useful to correct their diet is the OVERALL ENERGY REDUCTION. Furthermore, it would be desirable to associate with it:
- the decrease in portions of consumption, therefore a reduction in the volume of meals;
- The consumption of very little breakfasts, lunches and dinners, as the excess favors both the onset and the chronicity of symptoms.
- the drastic reduction (better the abolition) of spices, tea and coffee, these condiments / foods favor both the acidity and the pouring of the gastric contents inside the esophagus.
- The elimination of the components that REDUCE the tone of the LOWER ESOPHAGUS SPHINTER by worsening gastric containment and facilitating reflux; they are respectively: cocoa and / or chocolate, cigarette smoke and mint.
- It would also be desirable to follow the dietary advice useful for reducing gastric acidity, for example to moderate the portions of high-protein and hyperlipidic foods (both overcooked and undercooked), limit alcoholic beverages, pay attention to the digestibility of milk, etc.
Summarizing the guidelines for a "diet aimed at reducing the symptoms of GERD (also preventive against" esophagitis and Barrett's esophagus), we remind you that it is ESSENTIAL TO AVOID:
- Foods rich in fat
- Large portions in general and especially of high-protein and / or hyperlipidic foods, both overcooked and raw
- Coffee, tea, alcohol, carbonated and acidic drinks
- Chocolate, mint and spices
- Onion and garlic
- Very cold and very hot foods
- Hearty evening meals and milk before sleep
- To go to bed after meals
- To eat quickly while chewing little
- To perform physical exertion after meals
- To wear clothes and belts that are too tight after meals.
NB. Instead, it is RECOMMENDED to use chewin-gum as it can facilitate esophageal clearance by stimulating salivation and the frequency of swallowing.
A correct lifestyle can reduce symptoms in 20-30% of cases.
Bibliography:
- Gastrenterology manual for dieticians - National Coordination of University Teachers of Gastroenterology - Italian Gastroenterological Publishing - page 03:07