Generality
Anisocoria is the different amplitude of the two pupils, which can also be observed when they are exposed to the same degree of illumination. It may be a physiological anomaly, which need not be worried, or a sign of a morbid condition that requires immediate medical intervention.

Figure: Note the different diameter between the right pupil and the left pupil. From the site: wikipedia.org
Some of the more dangerous causes of anisocoria are: brain tumor, brain aneurysm, meningitis and severe head trauma.
The symptoms accompanying anisocoria are very varied and depend on the underlying pathological state (ie on the reasons that caused the anisocoria itself).
In order to cure anisocoria, the exact causes of the problem must be diagnosed; otherwise, or if you do not act promptly, the patient is in serious danger.
What is anisocoria?
Anisocoria is the different amplitude of the ocular pupils, which can also be observed in identical lighting conditions of the two eyes.
In other words, anisocoria occurs when the pupils, despite being exposed to the same amount of light, have different diameters from each other.
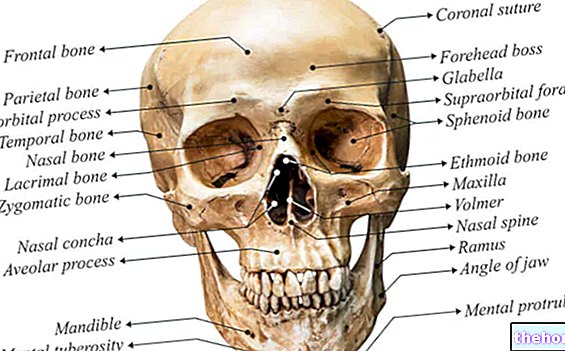
WHAT IS THE PUPIL?
The pupil of the eyes is a hole positioned in the center of the iris, which allows the light to hit the lens first and then the retina. The lens, in fact, is a lens that focuses on incoming light; the retina , on the other hand, it is the membrane located on the inner surface of the eye, which, thanks to the presence of photoreceptors (cones and rods), is sensitive to light and able to communicate with the brain via the optic nerve.
The diameter of the pupil varies according to the light present in the environment and which strikes the eye; these changes are regulated by a very precise muscle system, which is dependent on the third pair of cranial nerves (or oculomotor nerves).
The narrowing of the pupil occurs through the work of a muscle that surrounds the iris, called the constrictor muscle (or sphincter) of the iris; in bright light, this muscle narrows the pupil down to 1.5 millimeters.
The dilation, on the other hand, occurs thanks to muscles that are perpendicular to the constrictor muscle of the iris; these, in the dark, make the pupil widen up to about 8 millimeters in diameter.

View of the whole eye with an enlargement of the retina and the photoreceptors (or photoreceptor cells) that make it up. The nerve signal that regulates the constrictor muscle of the iris is of the parasympathetic type; vice versa, the nerve signal that governs the muscles responsible for dilating the pupil is of the sympathetic type.. From the site: webvision.med.utah.edu
WHAT DIFFERENCE MUST EXIST BETWEEN THE TWO PUPILS TO TALK ABOUT ANISOCORY?
In order to speak of anisocoria, there must be a difference of at least 0.4 millimeters between the two pupils.
A smaller deviation is not considered a noteworthy anomaly and cannot be classified as anisocoria.
Causes
Anisocoria can arise for different causes, being linked to particular morbid states but also to the intake of certain pharmacological substances or to singular health conditions. Furthermore, it is good to remember that some people with anisocoria do not have predisposing diseases or use drugs or toxic agents related to the disorder; in all these conditions we speak of physiological anisocoria.
Below is a list of the main causes of anisocoria.
- Physiological anisocoria. It has been calculated that about 20% of healthy people (i.e. without any nerve-ocular pathology and who do not take drugs or predisposing substances) have a significant difference (greater than 0.4 mm but less than a millimeter) between the two ocular pupils.
- Horner's syndrome. It is a disease caused by a defect in nerve transmission between the brain and the oculo-facial muscles on one side of the face only; it is mainly characterized by three signs: persistent myosis, ptosis of the eyelid and anhidrosis.
Persistent myosis is the condition in which the pupil remains narrow in diameter even in the absence of light; ptosis of the eyelid is the complete or partial lowering of the upper or lower eyelid (in fact, it is also called drooping eyelid); finally, anhidrosis is the inability to produce (or secrete) sweat which, in the case of of Horner, it can affect all half of the face involved or only a small part. - Traumatic events affecting the eye. A contusion in one eye, cataract surgery or eye inflammation (such as uveitis, narrow-angle glaucoma, etc.) can cause adhesion between the back of the iris and the front. of the lens; this can influence the mechanisms of narrowing and dilation of the pupil (at the level, obviously, of the eye involved). Anisocoria that has a traumatic origin is also called mechanical anisocoria.
- Adie's tonic pupil (or Adie's syndrome). It is a neurological disease characterized by a pupil that responds more slowly (than normal) to light stimuli. In other words, pupillary dilation and constriction occur with longer times than normal. Adie's tonic pupil mainly affects women.
- Paralysis of the oculomotor nerve. Oculomotor nerve palsy can be caused by a cerebral aneurysm, a blow to the head, an oculomotor nerve ischemia or a brain tumor. These conditions generally act by compressing the oculomotor nerve and affecting its normal functions.
- Pharmacological agents. Can cause anisocoria: eye drops based on pilocarpine or tropicamide, a cough medicine called dextromethorphan, alkaloids (for example scopolamine) contained in some plant species (genera Brugmansia And Datura) and, finally, some drugs such as cocaine and MDMA (Ecstasy).
- Meningitis. It is inflammation of the membranes (meninges) and / or cerebrospinal fluid (CSF) surrounding the brain and spinal cord. It can be triggered by infectious agents (viruses and bacteria) or non-infectious agents (sarcoidosis, systemic lupus erythematosus, etc.) .
- Migraine. It is a pathological condition characterized by unilateral headaches (i.e. on one side of the head only), which tend to worsen and are capable of causing intense and throbbing pain.
- Epilepsy. It is a neurological disease characterized by a "hyperactivity of some brain nerve cells.
Anisocoria, therefore, can be the sign of a serious pathology, which, if not treated immediately, can even lead to death.
Some causes of life-threatening anisocoria:
- Horner's syndrome, especially when it is caused by a carotid or jugular problem.
- Brain aneurysm
- Strong blow to the head
- Brain tumor
- Use of cocaine and MDMA
Symptoms
Physiological anisocoria does not cause particular symptoms or signs.
On the contrary, anisocoria related to certain morbid states or particular health conditions can be accompanied by:
- Blurred and / or double vision. It can be the consequence of a brain tumor, a cerebral aneurysm, a severe trauma to the head, an "ischemia affecting the oculomotor nerve or a" uveitis.
- Fever. It can occur in case of meningitis.
- Headache. It can be linked to several conditions: a meningitis, migraine, a brain tumor, a brain aneurysm or a severe trauma to the head.
- Confusion. It can be related to a brain tumor, a brain aneurysm, or a severe blow to the head.
- Loss of vision. It can be induced by a brain tumor, brain aneurysm, or oculomotor nerve ischemia.
- Sensitivity to light. It can be linked to Adie's syndrome, a cerebral aneurysm or an "ischemia that damages the oculomotor nerve.
- Nausea. It can result from a brain aneurysm, a migraine, a severe blow to the head or a brain tumor.
- Stiff neck. It can be the result of a brain aneurysm or migraine.
- Seizures. In addition to epilepsy, they can be due to a brain tumor, brain aneurysm or oculomotor nerve ischemia.
- Falling eyelid. It can mean not only Horner's syndrome, but also a brain aneurysm.
- Marked mydriasis. This may mean that you have oculomotor nerve palsy (for example from head trauma) or that you have been using cocaine.
WHEN TO SEE THE DOCTOR?

Figure: Person with Horner's syndrome. From the site: wikipedia.org
If the anisocoria appears suddenly or after a blow to the head, or if it is associated with severe pain in the head, it is best to contact your doctor immediately and be examined.
In the case of physiological anisocoria, a medical consultation is recommended if the difference between the pupils worsens markedly or one of the symptoms mentioned above is felt.
Diagnosis
Noticing a difference in diameter between the two pupils is quite simple, both for the doctor and for the patient with anisocoria himself (as it is sufficient for him to look in the mirror).
The most important thing to do, when a case of anisocoria arises, is to quickly establish what the causes may be; in fact, pupils of different diameters could be the consequence of a very serious and life-threatening condition.
Therefore, the patient is required to report to the doctor any symptoms experienced and any unusual events that may have occurred before the onset of the anisocoria (for example a blow to the head, trauma to an eye, etc.).
Without an exact diagnosis of the triggering causes, it is impossible to plan an adequate treatment; consequently, without appropriate and / or timely treatment, unpleasant consequences could occur.
DIAGNOSTIC TESTS
In addition to the physical examination, through which the doctor assesses the extent of the anisocoria and with what symptoms it presents, the patient may be subjected to:
- Blood exam completed.
- C reactive protein test, erythrocyte sedimentation rate (ESR) and leukocyte formula. There are three special blood tests, which allow you to measure the level of inflammatory markers in the bloodstream. They are useful in case of meningitis and in case of ocular inflammation.
- Lumbar puncture and cerebrospinal fluid analysis. It is particularly indicated in suspected cases of meningitis, as it allows to establish what are the triggering causes of inflammation at the level of the meninges.
- Eye drops test. It consists in "instilling" into the patient's eye, eye drops containing different pharmacological substances to study their effects on the pupil. It is very useful in case of suspected Horner's syndrome.
- CT scan (or computed axial tomography), nuclear magnetic resonance (or MRI) and X-rays of the head. There are three diagnostic imaging tests that can be used to identify a brain tumor, Adie's syndrome, a brain aneurysm, head trauma, damage to the oculomotor nerve, etc.
ANISOCORY IN DIFFERENT LIGHT CONDITIONS AND IN BRIGHT LIGHT CONDITIONS
For diagnostic purposes, it is useful to know that:
- Anisocoria that appears or is accentuated in poorly lit environments could be linked to Horner's syndrome or ocular trauma (mechanical anisocoria).
- The anisocoria that occurs mainly in the presence of intense light, on the other hand, could be a sign of Adie's syndrome, oculomotor nerve paralysis or a recent intake of certain pharmacological / toxic substances.
Treatment
The therapy to be adopted in the presence of anisocoria varies according to the triggering causes. For instance:
- If infectious meningitis is ongoing, antibiotic drugs or antiviral drugs should be given, depending on whether the underlying cause is a bacterium or a virus, respectively.
- If a tumor has formed inside the brain, surgery is needed to remove it.
- If the patient has suffered a severe blow to the head, it may be necessary to drain any hematoma that has formed inside the skull.
IN CASE OF PHYSIOLOGICAL ANISOCORY
For people with physiological anisocoria this is not provided and no treatment is required.
Prevention
Preventing anisocoria is somewhat complicated, because some conditions that cause it are also difficult to prevent (for example, brain tumor is a neoplasm that arises suddenly and without precise reasons).
If you practice jobs or sports in which it is possible to suffer trauma to the eye (therefore you are at risk of mechanical anisocoria), it is advisable to wear the most appropriate protections (helmets, etc.).
-corpi-estranei-e-altre-cause.jpg)