It is not yet clear what are the exact causes responsible for the onset of diabetic nephropathy and its evolution towards renal failure. Currently, it is assumed that some factors, including hyperglycemia, arterial hypertension and an altered cellular sodium transport, added to an innate genetic predisposition, are the main elements that favor the onset of diabetic nephropathy.
KEY CONCEPTS
At the kidney level, three fundamental processes take place in the two million nephrons present in approximately each kidney:
- filtration: takes place in the glomerulus, a highly specialized capillary system that allows all the small molecules of the blood to pass through the pre-urine, opposing only the passage of plasma proteins and blood cells
- reabsorption and secretion: they occur along the tubular system with the aim of reabsorbing from the pre-urine all excessively filtered substances (eg glucose, which the body cannot afford to lose in the urine) and to increase the " excretion of insufficiently filtered ones.
Due to various pathological processes (inflammatory, cicatricial, hypertensive ...) the glomerular sieve meshes can widen: the capillaries of the glomerulus thus let out normally retained blood components: this is the case of proteins, which consequently become found in excessive amounts in the urine. In this case we speak of proteinuria or macroalbuminuria (albumin is the main plasma protein).
Excessive filtration of glucose and proteins at the glomerular level causes progressive renal damage which progresses to renal failure. Below we describe the pathogenetic mechanisms that lead to the appearance of this damage.
The pathogenetic elements of diabetic nephropathy are represented by:
- Glomerular hyperfiltration: it is considered the first factor responsible for glomerulopathy in type I diabetes
- Structural alterations of the glomerular basement membrane: expression of microangiopathic damage that also occurs in other organs and systems
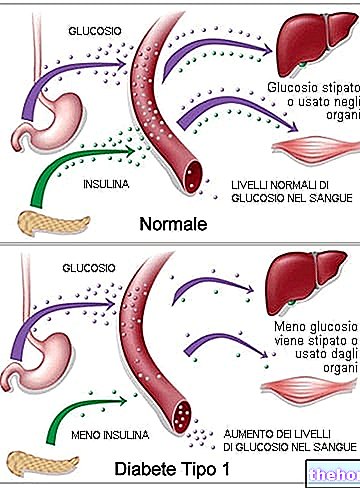
1) HYPERGLYCEMIA
↓
Increased filtration of glucose at the glomerular level
↓
Increased tubular glucose and sodium reabsorption
(The reabsorption of glucose at the level of the proximal convoluted tubule occurs through a Na + / glucose cotransport, so that there will be an increase in the volume and with it in blood pressure)
____________|____________
| |
Increase in blood volume and blood pressure
↓
stimulation of atrial stretch receptors with increased secretion of atrial natriuretic peptide ANP
↓
vasodilation of the afferent arteriole (to the glomerulus)
Reduction in the amount of sodium that reaches the macula dense
↓
vasodilation of the afferent arteriole and vasoconstriction of the efferent arteriole with release of antithrombin II|_______________________|
↓
increase in glomerular pressure and glomerular filtration rate
↓
responsible for the onset of nephrotic syndrome: initially selective proteinuria without hematuria + hypoalbuminemia and edema + hyperlipidemia and lipiduria
↓
functional overload of the nephrons with damage from wear and from activation of inflammatory phenomena → evolution towards chronic renal failure
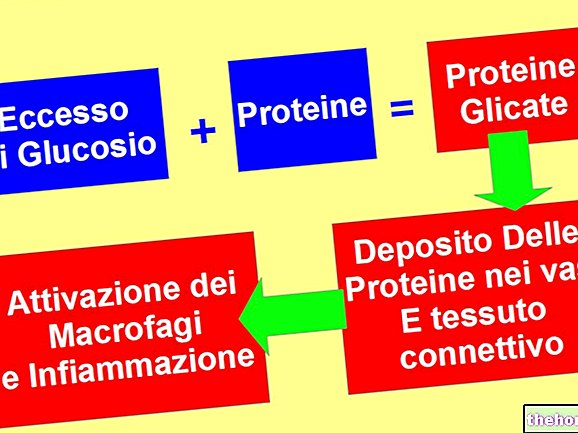
2) HYPERGLYCEMIA
_____________________________|______________________________
|
activation of the polyol pathway
||
formation of advanced glycation products
||
formation of oxygen free radicals
||
activation of the protein kinase C pathway
|___________________________________________________________
↓
increased vascular permeability and histological alterations with high synthesis of protein matrix at the glomerular level and subsequent sclerosis
↓
reduction of capillary permeability and filtering surface
↓
reduction of glomerular filtration rate up to renal failure
Watch the video
- Watch the video on youtube
Other articles on "Diabetic Nephropathy: Causes and Pathophysiology"
- Diabetic nephropathy
- Diabetic Nephropathy: Symptoms and Therapy

.jpg)