Risk factors
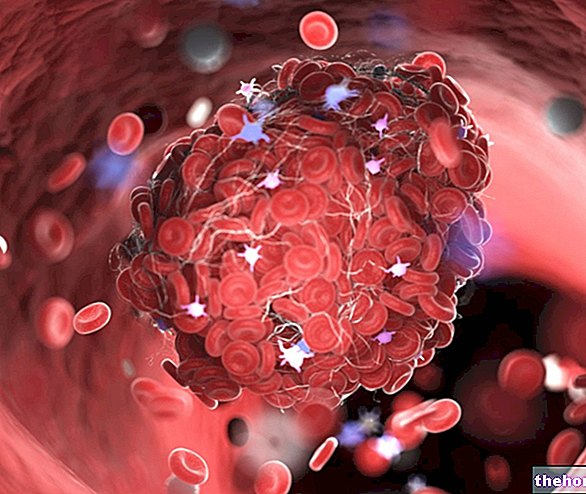
There are numerous elements capable of promoting the development of atherosclerotic plaques, the main cause of myocardial infarction.
The chances of having a heart attack are greater in people who:
- they smoke;
- have high blood pressure;
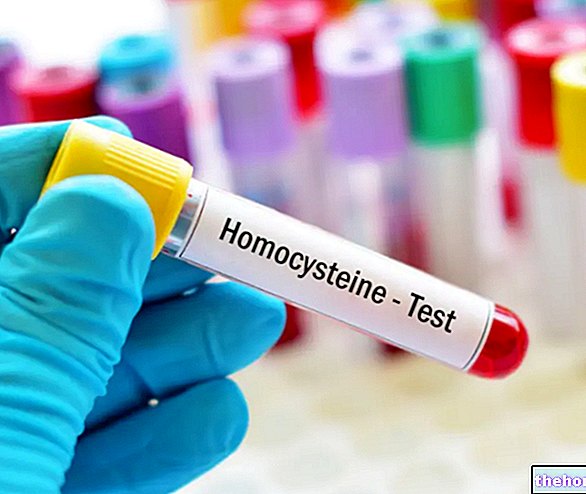
- have some abnormal blood values (elevated total cholesterol, increased LDL / HDL ratio, high triglycerides, elevated homocysteine, elevated C reactive protein, elevated fibrinogen, fasting hyperglycemia);
- are overweight or obese (especially if the fat mass is concentrated in the abdominal area);
- they have a sedentary job and do not engage in regular physical activity;
- make extensive use of alcohol and / or certain drugs (such as methamphetamines and cocaine);
- have one or more family members who have been affected by a heart attack (the risk increases if they have suffered the event at a young age, before the age of 60);
- they are male (it must be said, however, that the risk for women increases considerably after the age of 55 due to the loss of the protective effect exerted by estrogens during the fertile period);
- they are over 40 if men and 55 if women;
- they are highly stressed or are in a moment of physical or mental overwork (heart attacks often strike in the morning, the time of day when the highest levels of cortisol, also known as the stress hormone, are recorded).
Some risk factors cannot be removed, while all the others can be taken care of. The first are age, sex and family.
Sports and Heart Attack
Many cases of heart attack occur in conjunction with violent physical or mental exertion, with large variations in blood pressure.
For this reason, power activities (such as weight lifting) are on paper more dangerous than those of endurance carried out at medium-low intensity (running, swimming, cycling, cross-country skiing, etc.). healthy is perfectly capable of tolerating any kind of effort to which it is subjected and that physical activity is a very effective weapon in both primary and secondary prevention (ie to prevent the recurrence of a new heart attack). In the latter case it must obviously be structured according to precise directives and carried out under strict medical supervision.
Among the many benefits of physical activity there is also the strengthening of the so-called collateral circles, comparable to secondary roads capable of compensating, at least in part, for the reduced blood supply in the main road (coronary artery occluded by a thrombus).
Complications
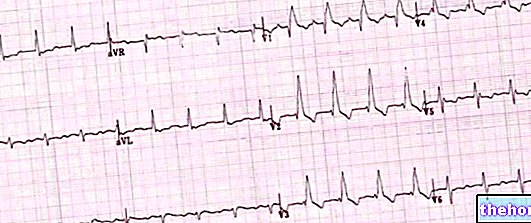
One of the most fearful consequences of myocardial infarction is represented by ventricular fibrillation, which is almost always lethal. Unfortunately this occurrence is not related to the extension of the infarction and even contained necrosis can be fatal due to the electrical instability they produce.
In practice, a heart affected by a heart attack can lose its fine and natural rhythm of contractions and relaxation, starting to beat in a very fast and disordered way (the ventricular muscle fibers, instead of contracting simultaneously, do it randomly, so the ventricle fails to pump blood into arteries and systemic circulation).
The only hopes, in these cases, are represented by a spontaneous resolution within a few seconds or by the rapid intervention of help, which - with the help of a cardiac defibrillator - can make the heart resume a physiological rhythm.
Another similar complication is represented by ventricular tachycardia, in which the rate of contraction becomes so fast as to significantly decrease the amount of blood released into the circulation and arterial pressure; all this can further aggravate the coronary ischemia and the extension of the heart attack. .
In some cases, the extent of tissue necrosis - determined by the heart attack - may be such that the heart is unable to pump adequate amounts of blood into the systemic circulation. The reduced blood supply to various organs can cause shortness of breath, weakness and swelling of the ankles and feet. This condition, known as heart failure, can be compensated if the myocardial contraction returns to be efficient in the following days or weeks (also thanks to the possible pharmacological support) or decompensated if the cardiac output does not return to normal levels.
There are significant dangers for patients who survived myocardial infarction, but who present with residual ischaemia, ventricular arrhythmias and left ventricular dysfunction. These complications can be treated with pharmacological and / or interventional therapy (angioplasty or bypass).
The weakness of the heart tissue affected by a heart attack can cause it to dilate excessively (ventricular aneurysm) in response to the pressure exerted by the blood inadequately expelled from the heart; in the most serious cases the damaged fibers can even break and in this case death often occurs rather quickly.
The lesions can also affect or disturb the functionality of the papillary muscles, which govern the correct functioning of the atrioventricular valves (mitral on the left and tricuspid on the right).
Other articles on "Heart Attack: Risk Factors and Complications"
- Heart attack
- Heart attack: diagnosis and treatment
- Heart attack - Drugs for the treatment of myocardial infarction
- Diet and heart attack

















-nelle-carni-di-maiale.jpg)




