ROLE OF THE PHYSICAL PREPARER IN VOLLEYBALL
In modern volleyball, the physical trainer can no longer limit himself to simply doing his job. Instead, it must be an essential point of reference for a whole system of relationships and interactions (with coach, doctor, physiotherapist, etc.).
The physical trainer must possess in his / her technical background knowledge relating to:
a) specific preparation of volleyball;
b) specific functional evaluation;
c) specific prevention (not only proposal of exercises performed correctly, but also evaluation of the stresses and protection of the athlete in carrying out the activity).
d) specific rehabilitation (knowledge such as to be able to help, but not replace, both the physiotherapist and the coach even with direct interventions on the field).

Team staff:
physical trainer
medical physiotherapist
2nd coach
1st coach
VOLLEYBALL PLAYER FUNCTIONAL ASSESSMENT TEAM
PHYSIOTHERAPIST
medical history
joint function
support and trim in orthostatic position (presence of insoles)
osteopathy evaluation
PREPARER
a) physical history
b) postural evaluation
c) muscle tension
d) body composition
e) flexibility and joint mobility
Physical history
Age (date of birth).
General anthropometric characteristics (height, weight, reach).
Specific circumferences (arm, upper-middle-lower thigh, calf).
Training habits (athletic experience of the player).
Past injuries (acute and chronic problems).
Postural evaluation
Presence of a kyphotic attitude (common in tall players).
Scoliosis and muscle deficit between the right and left side of the body.
Lumbar and hamstring tension (difficulty in flexing the torso).
Correct power position (shoulders open, paravertebral muscles contracted, center of gravity aligned on the supports).
Muscle tensions
Unbalanced training contents can lead to an imbalance between muscle groups that are functionally connected to each other, causing retractions and consequent muscle imbalances.
Any tensions must therefore be identified and quickly eliminated by analyzing the posture and symmetry of:
- head, shoulders, spine, pelvis and ankles (positioned behind the subject).
- cervical spine, dorsal spine, lumbar spine and abdomen (positioned sideways with respect to the subject).
Body composition
A fat athlete is not an athlete!
With a simple skin test it is possible to constantly monitor (every 6 weeks) the balance between fat mass and lean mass.
Personally I use eight folds (biceps, triceps, pectoral, subscapular, middle axillary, iliac crest, abdominal, anterior thigh), developing them in two formulas (Jackson & Pollock with seven folds, Durnin with four folds) and calculating the average between them.
Flexibility assessment
Functionality is associated with reading the athlete's posture. For this reason it is necessary, especially with younger athletes, to draw up a flexibility profile through three simple joint mobility tests:
- Sit and reach (Kendall figure)
- Squat test (various positions)
- Back rom test (sitting and supine)
THREE BASIC CONCEPTS
PREVENTION
Prevention means developing a system of physical work that prevents damage to the structures most stressed by technical training. Doing it well means reducing the risk and severity of injuries.COMPENSATION
To compensate means to re-establish a situation of equilibrium (in particular muscular) where the specific technical gestures tend to alter it. Doing it right means limiting muscle imbalances.REHABILITATION
Rehabilitating means bringing the athlete back to normal and complete sporting efficiency. Doing it well means avoiding the danger of relapses.
THE FACTORS OF PREVENTION
EXTERIOR
Footwear used
State of the pitch and training ground
Environmental conditions (temperature, humidity)
Role and competitive level of the athlete
INTERIORS
Recovery, integration and regeneration
Warm-up and cool-down
Workloads
Emotional stress
Training planning
Muscle balance
SPORTS REHABILITATION GUIDELINES
1) Reduction of the acute phase (inflammation etc.).
2) Recovery of movement (range of motion, correct walking, etc.).
3) Recovery of muscle strength and endurance.
4) Recovery of coordination and balance.
5) Recovery of sporting skills and specific athletic gesture.
Practical aspects of sports rehabilitation
Identify in which of the phases described above (not isolated but interconnected) the injured athlete is.
Determine the daily workload that the athlete can sustain, in order to avoid overload or underload.
To clarify well to the athlete the difference between biological healing and functional recovery, where by functional recovery we mean the recovery of the full technical-coordinative capacity of the gesture, the full maximum competitive potential and the full potential for mental finalization on the competition task.
Set up a preventive maintenance program after completing the return to competitive activity.
Work closely with physiotherapist, doctor and coach.
Stages of rehabilitation
1) Outpatient rehabilitation psychological support and setting of physical, manual, postural therapies etc.
2) Rehabilitation in water: range of motion, preparatory exercises for walking, toning and muscle strengthening performed in a protective environment.
3) Rehabilitation in the gym:
functional assessment test, general toning, walking recovery, aerobic work, proprioceptive exercises.
4) Rehabilitation in the field:
specific toning, coordination and dexterity programs.
PLEASE NOTE
Specific sports gestures tend to create imbalances in the muscles.
These imbalances, if not adequately compensated, lead to retractions that bring the joint heads closer and consequently determine a predisposition to joint pain.
Some muscles have a tendency to weaken and shorten, others just to weaken.
The correct compensation of the sporting gesture therefore becomes the first form of prevention for the sportsman.
PLEASE NOTE
In the analysis of the sporting gesture, the single muscular district is not evaluated, but the movement of the entire kinetic chain. For this reason, the solution to a physical problem can sometimes be found far from the sore spot.
Shoulder pain: ileo-psoas retraction.
Inguinal insertional pains: retraction of the hip flexors, leading to a forward displacement of the pelvis which in turn leads to a shortening of the adductors.
Back pain (lumbar area): retraction of the hip flexors and hamstring stiffness, factors that lead to hyperlordosis. Weakness of abs and buttocks.
Knee pain: retraction of the rectus femoris and imbalances between the flexors and extensors of the leg.
PREVENTION AND COMPENSATION EXERCISES IN VOLLEYBALL
Trunk and upper limbs (1st part)
Abdominals (rectum and obliques)
Spinal (dorsal, lumbar)
Lumbar and hamstring unloading postures
Traction + rower (ercolina)
Pull prone
Low pulley (pulled shoulders and arms)
Shoulder retroposition (prone decubitus, dumbbells)
Shoulder external rotation (dumbbells, arms extended)
Chest Pulled Lat Machine (Reverse Grip)
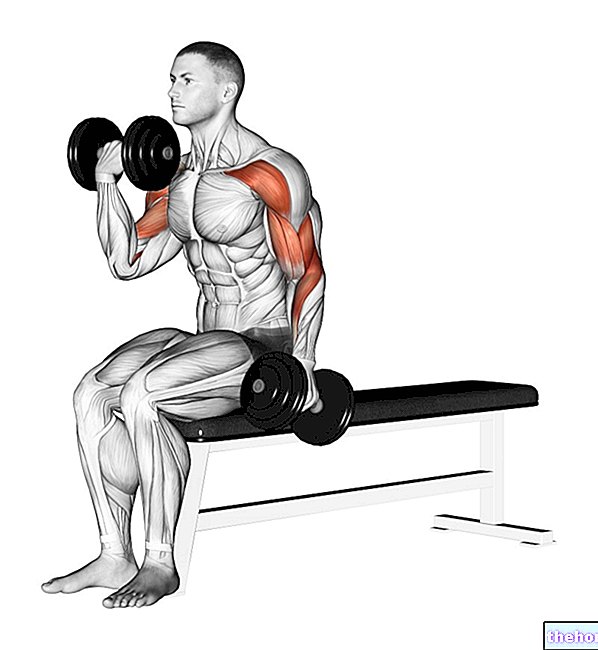
Trunk and upper limbs (2nd part)
Herculaneum extrarotation (short lever, ball under the arm)
Extra rotation with handlebar (lateral decubitus, short lever)
Outer rotator routines (light weight exercises)
Shoulder routine (elastic)
Lateral raises (dumbbells)
Raise forward palm down (dumbbell)
Baseball exercise with dumbbells
Lower limbs (1st part)
Isometric monopodalic leg extension (last grades, 6 "work + 1" rec.)
Eccentric monopodalic leg extension
1/3 isometric squat (6 "work + 2" rec.)
Eccentric monopodalic leg curl (assisted)
Eccentric monopodalic leg press
Single leg folded step
Split squats (multipower, dumbbells)
Sissy squat (2 dumbbells on the wall)
Lower limbs (2nd part)
Alternating front lunges (barbell, dumbbells)
Alternate side lunges (barbell, dumbbells)
Box squat (deep angle, with stop)
Dynamic parallel squat with medicine ball held between the knees
Sitting calf (slow eccentric phase)
Proprioceptive exercises (back, ankle, knee)
Electrostimulation
Other articles on "Prevention and rehabilitation in the palavolo"
- Resistance training in the sports hall
- Physical and rehabilitative medicine in volleyball