Generality
Zollinger-Ellison syndrome is a rare disease characterized by the presence of gastrinomas in the pancreas or duodenum.

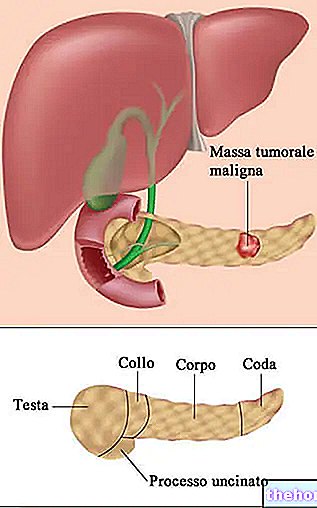
Figure: Illustration of a pancreas and duodenum during Zollinger-Ellison syndrome. From the pharmacy-and-drugs.com website
Gastrinomas are tumors, almost always malignant, which secrete significant quantities of gastrin. The presence, in the blood, of high levels of the gastrin hormone strongly stimulates the acid secretion of the stomach, giving rise to continuous peptic ulcers, severe abdominal pain, diarrhea, etc.
Diagnosis requires numerous tests, as different pathologies can cause the same symptoms as Zollinger-Ellison syndrome.
The best therapeutic solution is represented by surgery; however, this is feasible only under certain conditions. The possible alternatives are different, but almost always limited to the improvement of symptoms.
What is Zollinger-Ellison syndrome?
By Zollinger-Ellison syndrome we mean the set of signs and symptoms related to the presence of multiple peptic ulcers, due to gastric hyperacidity following the secretion of gastrin by one or more pancreatic and / or duodenal tumors, called gastrinomas.
Zollinger-Ellison syndrome is otherwise known as ZES, which is an acronym for English Zollinger-Ellison Syndrome.
Pancreas and duodenum
The pancreas is an exocrine and endocrine gland which, among other functions, also produces enzymes necessary for digestion.
The duodenum, on the other hand, is the first tract of the small intestine (or small intestine) and represents a fundamental collection point for digestive enzymes, which must intervene on the ingested food.
WHAT IS A GASTRINOMA AND WHERE DOES IT COME FROM?
Gastrinoma is an almost always malignant neoplasm, which originates from the so-called gastrin-secreting G cells, located in some areas of the stomach, duodenum and pancreas.
Gastrin is a peptide hormone which, once secreted, promotes the production of substances essential to the digestive process, such as hydrochloric acid and digestive enzymes.
EFFECTS OF GASTRINOMES
Gastrinomas induce a hypersecretion of gastrin → large quantities of this hormone make the stomach environment highly acidic → considerable gastric acidity causes peptic ulcers (erosions of the stomach and / or duodenum mucosa).
Peptic ulcers associated with Zollinger-Ellison syndrome mainly affect the duodenum and jejunum, which represent the initial and intermediate sections of the small intestine, respectively.
Other effects of gastrinomas:
- Increased levels of ACTH (adrenocorticotropic hormone)
- Increased levels of VIP (vasoactive intestinal peptide)
- Increase in glucagon levels
WHERE CAN GASTRINOMES FORM?
Gastrinomas that arise during Zollinger-Ellison syndrome are mainly located in the duodenum (60-65%) and pancreas (30%). However, they could also form in the lymph nodes adjacent to the aforementioned sites, in the stomach, liver, bile ducts, ovaries, heart and lungs.

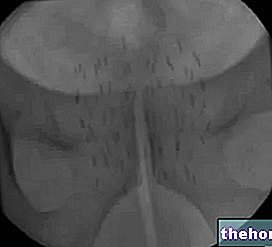
Figure: endoscopic image of a "peptic ulcer caused by an excess of gastrin. From the site en.wikipedia.org
If the gastric localization is explained by the presence, in the stomach, of G cells that secrete gastrin, the reasons that lead to the development of gastrinomas in the other minor sites remains unknown.
EPIDEMIOLOGY
SEZ is very rare: its annual incidence, in fact, is 0.5-2 cases per million people.
It mainly affects individuals between the ages of 30 and 50 and prefers the male sex.
Causes
Like all malignant tumors, gastrinomas are also the result of genetic DNA mutations. Specifically, the causes of these mutations are still unknown.
ASSOCIATION WITH MEN1
About 25% of patients with Zollinger-Ellison syndrome suffer from "another disease, called multiple endocrine neoplasia type 1 (MEN1)." The latter causes the appearance of tumors, called neuroendocrine, in the pituitary and endocrine glands. parathyroid.
Symptoms and Complications
For further information: Zollinger-Ellison Syndrome Symptoms
The characteristic symptoms of Zollinger-Ellison syndrome are abdominal pain and diarrhea.
With them, they can also appear very often:
- Nausea and bloody vomiting (or hematemesis)
- Acid reflux and persistent heartburn
- Sense of pain and discomfort in the upper part of the stomach
- Sense of weakness
- Weight loss due to a loss of appetite
- Malnutrition
- Anemia
WHEN TO SEE THE DOCTOR?
It is a good idea to consult your doctor in the presence of persistent abdominal or abdominal pain, accompanied by recurrent episodes of diarrhea, vomiting and nausea.
It is important not to overlook these disorders, as a disease such as Zollinger-Ellison syndrome, if diagnosed late, is difficult to treat successfully.
COMPLICATIONS
The recurrence of peptic ulcers, due to the continuous presence of acid secretions in the stomach, can cause gastrointestinal bleeding and perforation.
Furthermore, since gastrinomas are malignant tumors, there is a risk that they can spread metastases, especially in the liver.
N.B: metastases are cancer cells that have moved from their original location and moved elsewhere, contaminating the lymph nodes and / or other organs of the body.
Diagnosis
To be diagnosed, Zollinger-Ellison syndrome requires an elaborate test and procedure:
- Physical examination, during which the doctor evaluates the symptoms complained of by the patient and any clinical signs.
- Analysis of the patient's clinical and family history. Knowing if the suffering individual has, or has had, close relatives (parents or siblings) affected by MEN1 can be an important information, given the not rare association between the two diseases.
- Blood tests. They are used to measure gastrin levels in the blood (gastrinemia). If the gastrin is elevated it could be Zollinger-Ellison syndrome, but also other morbid conditions, such as gastric atrophy, renal failure, pheochromocytoma or pernicious anemia. reasons of a high gastrin.
- Stimulation test with secretin. The intravenous injection of secretin (a peptide hormone also secreted by the body to reduce the acidity of the stomach that is too high) causes, in individuals with ZES, a very particular reaction, which basically consists of a sudden increase (NB: in no more 30 minutes) of gastrin levels in the blood.
- Upper gastrointestinal endoscopy. It consists in "introducing, in the digestive system of the patient, an instrument equipped with a light and a camera, capable of showing the internal aspect of the stomach and duodenum. Thin and flexible, this instrument, which is called an endoscope, also offers the possibility of take a sample of cells for a biopsy.
During the examination, the patient is conscious but sedated. - CT (Computed Axial Tomography), MRI (Nuclear Magnetic Resonance), Ultrasound and Somatostatin Receptor Scanning (SRS). They are used to identify the exact location of gastrinomas and their appearance (single, multiple, etc.).
- Endoscopic ultrasound. It consists of inserting an ultrasound probe into the digestive tract in order to examine the stomach and duodenum and possibly also take a tissue sample for a biopsy examination.
- Measurement of chromogranin A. Chromogranin A is a marker of neuroendocrine tumors, such as those caused by MEN1.
Gastrin levels in the blood (unit of measurement is the picogram / milliliter, or pg / mL)
- Normal person: not exceeding 200 pg / mL
- Person with ZES: at least 1,000 pg / mL
Treatment
In the case of Zollinger-Ellison syndrome, surgical removal of gastrinomas is the best therapeutic solution. However, the conditions do not always exist to be able to put this type of intervention into practice.
The alternative solution is to treat the disease as if it were a "peptic ulcer, then giving the patient proton pump inhibitors (PPIs) and H2 blockers (H2 blockers). The administration of these drugs only acts on the symptoms, relieving them, but it does not make the tumors regress and does not protect the patient from the possible spread of metastases.
Liver metastases can be removed with a "surgical operation only if the malignant cells, which have reached the liver, are concentrated in a" circumscribed area and are not found in depth.
HOW AND WHEN TO OPERATE?
Gastrinomas are surgically removable, through a laparoscopic or laparotomy operation, provided they are single and well localized. impractical solution.
Alternatively, but only in certain situations, it is possible to try to solve the problem with one of the following treatments:
- Surgical removal limited to the largest gastrinoma.
- Embolization. The doctor cuts off the blood supply to the area where the tumors reside, thus causing the cancer cells to die.
- Destruction of tumor cells by radiofrequency ablation.
- Chemotherapy and / or radiotherapy.
THERAPY BASED ON IPP AND ANTI-H2
Proton pump inhibitors (PPIs) and H2 blockers (H2 blockers) reduce acid production in the stomach, relieving symptoms caused by massive gastrin production.
Such drugs are effective, but only when taken in large doses and for prolonged periods.
Long-term treatment with PPI and H2 blockers can cause serious side effects in people over the age of 50, such as: hip, wrist and / or vertebrae fractures.
Most used IPPs:
Most used H2 blockers:
- Esomeprazole
- Lansoprazole
- Omeprazole
- Pantoprazole
- Rabeprazole
- Ranitidine
- Nizatidine
IN CASE OF METASTASIS IN THE LIVER
If liver metastases are concentrated only in a single area of the liver and isolated from the rest of the organ, it is possible to remove them surgically.
In the absence of these conditions, the only viable remedy is liver transplantation, a delicate operation that is not without possible complications.
OTHER TREATMENTS
If peptic ulcers perforate the stomach, specific intervention is required.
If they cause severe blood loss, on the other hand, an immediate blood transfusion is needed to remedy the anemia.
Prognosis
If the diagnosis is timely, there are greater chances of intervening with a surgical operation (as the tumor could still present itself in a single form) and definitively cure the patient.
In cases in which the gastrinoma is not removed in time, is located in a location that is difficult to access, or is associated with MEN1, the "surgical intervention becomes a" very remote hypothesis, for which the patient is forced to live with the symptoms typical of Zollinger-Ellison syndrome (peptic ulcers, diarrhea, etc.).