Generality
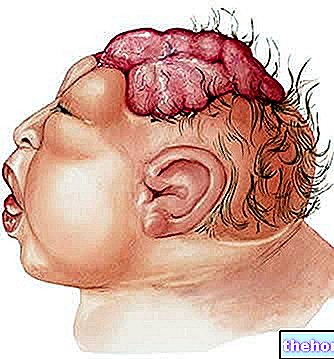
The omphalocele is a congenital anatomical defect, characterized by the failure to close the abdomen and the consequent protrusion, through an opening at the umbilical level, of one or more abdominal organs (intestine, liver, stomach, spleen, etc.).

From: https://en.wikipedia.org/wiki/Omphalocele
In a more than fair number of cases, omphalocele represents a clinical sign of specific chromosomal alterations, such as those that induce trisomy 13 or trisomy 18.Furthermore, the correlation between omphalocele and congenital defects of the heart and / or neural tube is frequent.
Doctors can diagnose omphalocele already during prenatal life, by means of some special tests.
The only feasible therapy is of the surgical type and consists in the re-insertion of the extra-abdominal organs in their ideal cavity.
What is the omphalocele?
The omphalocele is a congenital defect of the abdominal wall, characterized by the protrusion, through a more or less wide opening at the umbilical level, of the main organs of the abdomen (ie liver, intestine, stomach, etc.).
Typically, around these protruding organs, there is a thin, transparent serous membrane, much like a sac, which arises from an ejection of the peritoneum. This bag is usually intact.
According to doctors, omphalocele is a special type of hernia.
A "hernia is the leakage of a bowel, or part of it, from the cavity that normally contains it (N.B: the word bowel indicates a generic internal organ).
Causes
Brief introduction: under normal conditions, until about the tenth (X) week of pregnancy, the intestine of the fetus resides outside the abdomen, just outside the navel. After that, the abdominal cavity absorbs it, through a process of fusion of the abdominal muscle wall.
At the origin of "omphalocele c" is an incorrect development, during fetal life, of the abdominal muscles. These elements, in fact, instead of merging with each other and absorbing the intestine, remain separate and give rise to a real opening on the belly .
With the continuation of the pregnancy and the enlargement of the size of the fetus, also abdominal organs such as the stomach or liver gradually tend to protrude and to find themselves, in a completely abnormal way, outside the abdomen.
As will be seen, there are cases of omphalocele that are more serious than others.
ONPHALOCELE AND CHROMOSOMAL ANOMALIES
In a fair number of cases (about 15%), the omphalocele coincides with the presence of some specific chromosomal anomalies.
Chromosomal abnormalities are serious genetic conditions, characterized by numerical and sometimes even structural alterations of the chromosomes, that is, the cellular elements in which DNA resides.
This coincidence has led doctors and experts to believe that the two circumstances are closely connected with each other, with the omphalocele representing a clinical manifestation of the chromosomal anomaly present.
The chromosomal anomalies that most frequently determine the presence of omphalocele in those who carry it are trisomy 18 (or Edwards syndrome), trisomy 13 (or Patau syndrome) and Beckwith-Wiedemann syndrome.
What are trisomy 18 and trisomy 13? A few details
Geneticists speak of trisomy when the genetic makeup of an individual has three chromosomes of the same type, that is, a triplet of homologous chromosomes, rather than a pair (as it normally should be). Therefore, if the total number of chromosomes in any single cell of a healthy person is 46, the total number of chromosomes in any single cell of a person with trisomy is 47.
Trisomies are part of those genetic abnormalities known as aneuploidies, i.e. changes in the chromosome number.
Carriers of trisomy 18 and trisomy 13 have three copies of autosomal chromosome 18 and three copies of autosomal chromosome 13, respectively.
In both cases, their health conditions are very serious and often incompatible with life. In fact, if death has not already taken place in the prenatal age, it is very likely to occur shortly after birth.
Both trisomy 18 and trisomy 13 are responsible for characteristic physical alterations (especially at the facial level) and include, as the only known risk factor, the advanced age of the mother.
EPIDEMIOLOGY
According to some estimates by the United States Center for Disease Control and Prevention (CDC), in the United States, the annual frequency of omphalocele is 2-2.5 cases per 10,000 new births.
Also according to the same research, the mortality rate linked to this abdominal wall defect would be around 25%.
Symptoms and Complications
For further information: Omphalocele Symptoms
The characteristic sign of omphalocele is the extra-abdominal presence (ie external to the abdomen) of the organs that should normally be located inside the abdominal cavity.
Not all omphaloceles are equally severe. Their severity depends on the size of the opening on the abdomen and on how many organs protrude outside it.
Therefore, doctors consider an omphalocele characterized by protrusion of only the intestine to be small (or of limited severity); while they consider an omphalocele characterized by protrusion of the intestine, liver, spleen, etc. as large (or of high severity).
OTHER SIGNS
Often, the abdominal cavity of babies with omphalocele is much smaller than it really should be. As will be seen in the chapter on therapy, this represents a problem when the doctor intervenes surgically.
COMPLICATIONS
Being virtually unprotected (N.B: the peritoneum does not provide a particularly efficient defense), the abdominal organs located outside the belly can:
- Easily develop an infection. Infections are particularly common when the peritoneum ruptures.
- Easily receive pinching or twisting. All this can damage the affected organ and cause a large and very dangerous blood loss.
ASSOCIATED DEFECTS
Often, babies with omphalocele are born with heart defects and neural tube defects (i.e., the embryonic structure from which the central nervous system originates).
These alterations may be the result of the associated chromosomal abnormalities, described above, or of other causes, in many cases, unknown.
The simultaneous presence of omphalocele and other defects in other apparatuses or systems reflects a very serious health condition, fatal within a few days (if not even in the prenatal phase).
Type of defect
Percentage
Congenital neural tube defects
40%
Diagnosis
At birth, the diagnosis of omphalocele is quite simple. The newborn, in fact, has clear and unambiguous signs.
In the prenatal phase, however, doctors could detect the presence of the abdominal defect through a normal ultrasound.
In these situations, the ultrasound examination must be followed by more in-depth checks, which serve to establish the severity and characteristics of the omphalocele, any other congenital anomalies and the chromosomal structure of the fetus.
To clarify all these aspects, doctors resort to:
- Level II ultrasound
- Fetal echocardiography
- Amniocentesis and / or fetal karyotype
LEVEL II ULTRASOUND
The second level ultrasound is a more precise examination than the simple prenatal ultrasound (level I ultrasound). In fact, it provides very clear images of the fetal organs (and any anomalies) and allows you to understand how the development of the fetus is proceeding inside the uterus.

FETAL ECHOCARDIOGRAPHY
Fetal echocardiography is a normal ultrasound of the heart, which allows you to analyze the anatomy, function and rhythm of the fetus' heart. Therefore, it is useful to clarify whether the newborn has cardiac alterations associated with the omphalocele.
It is carried out by a doctor who specializes in fetal and pediatric cardiology.
AMNIOCENTESIS
Amniocentesis consists in the transabdominal removal of a small quantity of amniotic fluid.
Contained within a sac (amnios or amniotic sac), amniotic fluid is the fluid that surrounds and protects the fetus during its uterine development.
Once the sample has been taken (N.B: doctors generally perform amniocentesis between the 16th and 18th week of pregnancy), the analysis laboratory carries out various tests on the sample obtained, including a check of the chromosomal set.
Therefore, amniocentesis allows us to understand if the omphalocele is associated with some particular chromosomal alterations.
FETAL KARYOTYPE
The fetal karyotype is a highly specific evaluation test of the chromosomal set of the fetus (N.B: higher than amniocentesis), which allows to accurately probe all the chromosomes of a collected cell sample.
This makes it possible to identify the smallest chromosomal alterations, which a less precise examination, such as amniocentesis, is not always able to detect.
IN CASE OF PRENATAL DIAGNOSIS
If the diagnosis of omphalocele occurs in the prenatal phase, the mother must undergo periodic monitoring, through which the doctor observes the progress of the pregnancy.
It is not excluded that the omphalocele regresses spontaneously during gestation.
Treatment
The treatment of the omphalocele is exclusively of a surgical type and has as its final aim that of reinserting, inside the abdomen, the organs that reside outside it.
The possibility of applying this therapy depends mainly on two factors:
- The severity of the omphalocele. The more severe it is, the more difficult the intervention.
- The congenital anomalies that accompany the omphalocele. The more and more serious they are, the more attention and additional care that must be given to the little patient.
ONPHALOCELE OF SLIGHT GRAVITY AND ISOLATED
If the omphalocele is small in size (for example, when only the intestine is outside the abdomen) and is not associated with other pathologies, doctors have a good chance of successfully completing the replacement surgery.
Generally, the operation is never immediate, but always occurs after a short period of time after birth. During this time, the surgeon who will operate the baby covers the omphalocele with a special synthetic material.
From an executive point of view, the intervention is rather delicate and requires considerable competence and experience from the entire medical staff.
Reasons for the good chance of success
Reinserting just one organ is easier than reinserting two or more.
In addition, infants with mild omphalocele often have a normal-sized abdominal cavity that is no smaller than normal. Thanks to this, the feasibility of the operation is greater.
SEVERE AND VERY SEVERE ONPHALOCELE
If the omphalocele is severe or very severe, because it is associated with other congenital defects, doctors generally have little chance of successfully treating (or even intervening on) the protrusion of the abdominal organs.
The reasons are different. First, most newborns in this state have a very small abdominal cavity, which does not guarantee the space that the extra-abdominal organs need. Secondly, congenital defects, such as congenital anomalies, are situations that make the "execution of a" surgical operation contraindicated.
Sometimes, it may happen that there are no foundations to operate only in the first years of life. In such circumstances, doctors choose to postpone surgery to childhood, in the hope that the abdomen will expand its internal space in the meantime.
What is the type of delivery in case of severe or very severe omphalocele?
In the case of severe or very severe omphalocele, doctors resort to giving birth by caesarean section, because it is less dangerous for both the mother and the fetus.
Prognosis
According to what was said in the previous chapter dedicated to therapy, the prognosis of omphalocele depends on its severity and the associated pathologies.