Generality
Adrenal insufficiency is a condition in which the endocrine activity of the adrenal glands appears to be severely compromised, to the point of being insufficient with respect to the needs of the organism.

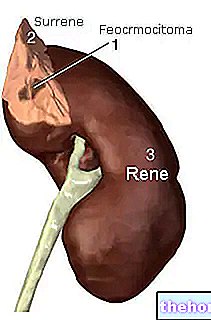
The adrenal glands are two small glands located in the adipose tissue that covers the upper portion of the kidneys; they are essential for the synthesis of three hormonal classes, that of androgens (less important because it is flanked by gonadal synthesis), that of glucocorticoids (led by cortisol) and that of mineralocorticoids (led by "aldosterone).
Symptoms
For further information: Adrenal insufficiency symptoms
It is precisely the lack of one or more of these hormonal classes that determines the characteristic symptoms of adrenal insufficiency; this condition typically manifests itself with hypoglycemia, dehydration, hypotension, dizziness (especially when rising suddenly from a sitting or lying position) weight loss, confusion, weakness, nausea, diarrhea, darkening of the skin and an excessive need for salty foods.
The same symptoms are also typical of Addison's disease, which is not surprisingly the most common cause of primary adrenal insufficiency.
Due to the lack of androgens, a reduction in pubic and axillary hair and a decrease in libido (sexual desire) can also be appreciated in women,
Often, adrenal insufficiency sets in gradually, with faded and slowly worsening symptoms that make early recognition of the disease very difficult.
On the other hand, the clinical manifestations of "adrenal insufficiency are accentuated in conditions of severe stress, such as an accident or a serious infection, to the point of being lethal in the absence of adequate treatment; in these cases we speak of" Addisonian crisis "or acute adrenal crisis.
Causes
Primary Adrenal Insufficiency
The primary forms of adrenal insufficiency are due to intrinsic damage of the adrenal gland, which in spite of an increased level of ACTH fails to produce adequate levels of cortisol; in these cases we speak of Addison's disease. Most episodes (75-80%) are sustained by extensive damage to the adrenal parenchyma on an autoimmune basis (abnormal antibodies directed against organ cells); in these cases, hypoadrenalism is very often accompanied by other pathogenic diseases autoimmune; frequent is the association with chronic thyroiditis (Hashimoto's disease), type I diabetes mellitus, premature ovarian failure or with skin problems (alopecia and vitiligo). The infectious etiology and in particular the tuberculous etiology have less importance today than in the past, with a higher incidence in developing countries. Among the other causes of primary adrenal insufficiency we remember adrenal tumors, metastases and haemorrhages adrenal, amyloidosis, hemochromatosis, developmental anomalies of the adrenal glands and infections of various kinds.
Secondary adrenal insufficiency
The secondary forms of adrenal insufficiency are due to a pituitary problem, that is localized at the level of the small gland at the base of the brain and responsible, among other things, for controlling adrenal activity through the release of adrenocorticotropic hormone (ACTH). This hormone acts as a powerful stimulus to adrenal activity, which in its absence is deficient, to the point of causing hypotrophia of the organ. The secondary forms of adrenal insufficiency are far more common than in cases of Addison's disease; they are often temporary, due to abrupt discontinuation of prolonged cortisone therapy or surgical removal of ACTH-secreting tumors.
More rarely, secondary adrenal insufficiency is linked to pituitary tumors, to radiation therapy undertaken to defeat them, to surgical removal of the gland or to its hemorrhagic or infectious processes.
The fundamental symptomatological difference compared to the primary forms is the lack of browning of the skin, given that the levels of ACTH are lower than normal. Furthermore, the clinical symptoms are generally more nuanced, since the production of the mineral-active hormones (aldosterone) is preserved; however, additional disturbances due to the lack of other pituitary hormones may coexist, with menstrual changes, infertility, impotence, pubertal delay and failure to thrive in children.
Tertiary Adrenal Insufficiency
Finally, rare tertiary forms of adrenal insufficiency can also be recognized; in this case the problem is localized in the hypothalamus, which does not release enough CRH hormone (which in normal conditions stimulates the pituitary to secrete ACTH, see figure).
Diagnosis
The diagnosis of adrenal insufficiency is based on blood and urinary tests aimed at assessing hormone levels (cortisol, aldosterone, ACTH and renin), but also minerals such as sodium and potassium (aldosterone favors the reabsorption of the former and the excretion of the latter. ).
CT and magnetic resonance imaging can be performed to investigate the anatomy of the adrenal glands and the hypothalamus-pituitary region.
Care and Treatment
See also: Drugs for Adrenal Insufficiency
The treatment of adrenal insufficiency is a substitute and as such based on the administration of the synthetic forms of hormones produced by the adrenal gland. The goal of treatment is to eliminate the symptoms of hormone deficiency without inducing those of excess, while maintaining a balance that protects the patient from the Addisonian crisis.
In the primitive forms (Addison's disease) it is necessary to administer both glucoactive and mineralactive drugs; the latter are not used in the secondary and tertiary forms, as the ACTH deficiency does not affect the synthesis of aldosterone (which is instead controlled by the renin-angiotensin system). It is essential that the therapy is never self-suspended by the patient and that in the event of stressful events (illness, surgery, etc.), or when oral introduction is not possible, the cortisone dosage is increased or replaced with intramuscular or intravenous administration.
Treatment, in most cases, lasts a lifetime. With adequate therapy and a few small precautions, people with adrenal insufficiency can lead a normally active life and enjoy the same life expectancy as the healthy population.
Some forms of adrenal insufficiency, however, recognize a treatable cause: tuberculosis and other infections, for example, can be treated specifically; analogously if the adrenal gland does not receive enough blood or, on the contrary, is the site of hemorrhage.
Finally, rapid intravenous administration of hydrocortisone, glucose and saline is required in episodes of acute adrenal crisis (addisonin crisis).