Klinefelter's syndrome is a genetic disease that affects only males. What characterizes this disease is the presence of an extra X chromosome. This chromosome does not allow, during puberty, the normal development of purely male sexual characteristics.

Figure: Shows a summary of the main clinical manifestations of Klinefelter's syndrome. From hypogonadism to typically female physical characteristics (wide hips, gynecomastia and narrow shoulders), from mental retardation to diabetes mellitus.
Unfortunately, there is no specific cure. However, some therapeutic treatments reduce the most severe symptoms and consequently improve patients' quality of life.Human chromosomes
Each cell of a healthy human contains 23 pairs of chromosomes. One pair of these chromosomes is of the sexual type, that is, it determines the sex of the individual; the remaining 22 pairs, on the other hand, are composed of autosomal chromosomes. In all, therefore, the human genome has 46 chromosomes.
ALTERATIONS OF GENES
Each pair of chromosomes contains certain genes.
When a mutation occurs in a chromosome, a gene can be defective. This defective gene, therefore, expresses a defective protein.
Conversely, when the number of chromosomes varies, we speak of aneuploidy. In this case, instead of two, the chromosomes can be three (trisomies) or only one (monosomy).
THE SEXUAL CHROMOSOMES
Sex chromosomes are key in determining a person's sex, male or female. The woman has two copies of the so-called X chromosome in the cells of her body; the man, on the contrary, has an X chromosome and a Y chromosome. As for the autosomal chromosomes, also the sexual ones are inherited from the parents: one copy is donated by the father, another one from the mother.
There are several genetic diseases due to the sex chromosomes. They present either alterations in the chromosomal structure, or modifications in the number of chromosomes. Among the latter, in addition to that of Klinefelter, we remember the turner syndrome, the trisomy X syndrome and the double Y syndrome.
What is Klinefelter's syndrome
Klinefelter syndrome is a genetic disease of the male sex characterized by the presence of a third sex chromosome (trisomy). This chromosome is of type X. The cells of patients with Klinefelter's syndrome therefore have a chromosomal set of 47, XXY.
Men with an extra X chromosome have:
- Abnormalities in the testicles (the male gonads), also called testicular dysgenesis.
- Underdeveloped secondary sexual characteristics.
- Female somatic characters.
EPIDEMIOLOGY
Klinefelter syndrome affects one boy for every 500 new births. The data is, however, uncertain. In fact, other estimates speak of one case for every 1,000 new births. This uncertainty is due to the fact that some mild forms of the disease go unnoticed, as they result in almost imperceptible signs and symptoms.
Additionally, out of every 100 infertile males, 3 have Klinefelter's syndrome.
Causes
The abnormal presence of an extra sex chromosome of type X causes Klinefelter syndrome in males. It should be noted that this is a "non-hereditary genetic anomaly. The parents, therefore, are healthy.
So why are some sons born with an extra X chromosome?
PATHOGENESIS
The answer, from a genetic-biological point of view, is very complex. It seems that the genetic error begins during meiosis or during mitosis of the fertilized egg, ie the embryo.
Meiosis is the process by which some cells in the body with 46 chromosomes divide into 4 sex cells with 23 chromosomes each. These cells are the spermatozoon, for the man, and the egg cell (oocyte), for the woman. The union of an egg cell with a spermatozoon gives rise to the fertilized egg, with 46 chromosomes (23 + 23).

Figure: shows the nondisjunction process during meiosis. One of the four nascent cells carries both chromosomes with it. If this cell is the one that will fertilize the egg (or is the egg itself), then there will be a genetic anomaly.
Mitosis is the division of a parent cell into two identical daughter cells, with a complete chromosome set.
The genetic error consists in the non-separation (or non-disjunction) of one of the chromatids, ie the chromosomes in the duplicated form. Therefore, when the cells divide:
- In meiosis, a sex cell will have a number of chromosomes equal to 24 chromosomes.
- In mitosis, a daughter cell will have a number of chromosomes equal to 47 chromosomes.
In the case of Klinefelter syndrome, this additional chromosome is the X chromosome.
GENETICS: XY / XXY MOSAICISM
Some patients with Klinefelter syndrome possess a completely 47, XXY genome. Other patients, on the other hand, have a mixed genome: 47, XXY and 46, XY.In this case we speak of genetic mosaicism.
What is the explanation for all this?
It all depends on the moment in which non-disjunction occurs.
If it occurs during meiosis, the genome is totally 47, XXY. In fact, the egg cell, or the spermatozoon, immediately have an altered number of chromosomes.
The genome, on the other hand, is mixed, when non-disjunction occurs during mitosis of the fertilized egg. In this case, the sperm and egg cell, at the time of fertilization, have a normal number of chromosomes. The error of non- separation occurs during the division of embryonic cells. Result: at the end of embryonic development, some cells will have 46 chromosomes, others 47.
Subjects with an XY / XXY genome usually have less symptoms than those with a totally 47, XXY genome.
GENETICS: OTHER VARIATIONS
Although rarely, patients have been observed with a chromosome set consisting of more than 2 X chromosomes. For example:
- 48, XXXY
- 49, XXXXY
- 48, XXYY
- 49, XXXYY
The presence of such genomes is very rare and often coincides with severe forms of intellectual deficit and multiple physical malformations.
Symptoms
For further information: Symptoms of Klinefelter Syndrome
The first symptoms of Klinefelter syndrome appear during puberty, affecting its normal evolution. The pubertal process, in fact, undergoes a slowdown and an early termination. The main clinical manifestations are hypogonadism (ie small testicles) and an altered maturation process of the spermatozoa (spermatogenesis).
In the pre-pubertal age (childhood and pre-adolescence), only some patients show signs that lead to suspicion of Klinefelter syndrome. These are rather vague manifestations, because they are common to other pathological circumstances or because they are not so evident as to attract the attentions of family members.
POSSIBLE PREMONITORY SIGNS OF THE PREPUBERAL AGE
The deficits found in this growth phase can be:
Mental delay
The musculature is weaker than the peers
Difficulty speaking and delivering a speech
Delay in taking the first steps
Lack of coordination
Difficulty in reading
Patients tend to be introverted and unsure of themselves. They appear immature compared to their peers
AFTER THE PUBLICATION €
At this time in life, the symptoms of Klinefelter's Syndrome become evident. The main clinical symptoms are:
- Alteration of spermatogenesis
- Complete absence of spermatozoa (azoospermia)
- Maturing of testicles
- Spermatogenesis
- The production of testosterone.
- Face
- Pubis
- Armpits
30%
> 45%
In addition, the physical appearance also takes on specific characteristics:
- Obesity
- Tall stature
- Upper and lower limbs elongated and out of proportion to the rest of the body
- Physiognomy of the body similar to that of a woman (narrow shoulders and wide hips)
PSYCHOLOGICAL ISSUES, PSYCHOLOGICAL PROBLEMS
The psychological aspect deserves a separate chapter. Patients with Klinefelter syndrome suffer from depression. In fact, they perceive the differences from healthy peers and consequently respond with attitudes characterized by:
- Introversion
- Subditance
- Anxiety
Hypogonadism, lack of libido and gynecomastia have the greatest influence on the psyche of Klinefelter's syndrome patients.
COMPLICATIONS
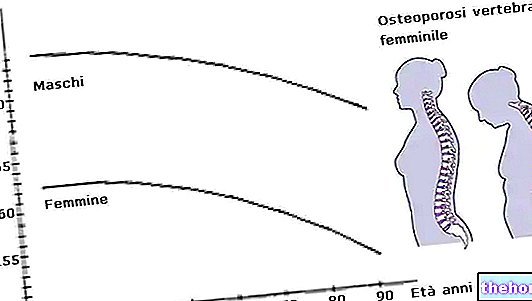
They are mainly due to hormonal disturbances, which affect testosterone. In fact, the lack of testosterone synthesis increases circulating cholesterol levels in the blood and promotes osteoporosis. Furthermore, males with Klinefelter syndrome are more affected than healthy males by breast cancer.
Finally, the association with diabetes mellitus is very common.
Due to hypercholesterolemia
Testosterone treatment lowers cholesterol levels
Due to Gynecomastia.
The risk is much higher in healthy males
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Sjogren's syndrome
- Thyroiditis
Diagnosis
To trace the presence of an extra X chromosome, a genetic test known as a karyotype is used.
KARYOTYPE

Figure: the chromosomal makeup of a patient with Klinefelter syndrome, observed with the karyotype test.
It consists in the analysis of the chromosomal set of an individual.
The karyotype reveals if there are variations in the normal number of chromosomes. It can be performed on a sample of amniotic fluid, for a pre-natal diagnosis of the disease, or on a blood sample, for a post-natal diagnosis.
As mentioned, puberty represents the crucial moment for the onset of symptoms of Klinefelter's syndrome. In the earlier stages (pre-natal and pre-pubertal age), the karyotype is the only diagnostic test useful for detecting Klinefelter's syndrome. When performed, it is very often for fear of other pathologies.
After pubertal development, the karyotype confirms the pre-diagnosis, based on the signs.
OTHER USEFUL EXAMINATIONS
Alongside the karyotype, there are other very useful and indicative investigations of the disease. They consist of blood and urine tests, testicular biopsy and bone densitometry.
Below is a table indicating the test, why it takes place and how invasive it is.
- Gonadotropins (higher than normal)
- Testosterone (lower than normal)
- Gonadotropins (higher than normal)
- Alterations of spermatogenesis.
- Possible oligozoospermia or azoospermia
Yes. Minimally invasive, it is surgery; requires local anesthesia; it does not require post-operative hospitalization.
- Osteoporosis
Finally, some evaluations of the physical-anatomical aspect should not be forgotten, such as:
- The small size of the testicles (hypogonadism).
- The minor hair development of the face, armpits and pubis.
Therapy
As this is a genetic disease, there is no cure that solves the root problem. However, some therapeutic measures can be applied, useful for:
- Correct and limit hypogonadism
- Reduce the effects of gynecomastia
- Promote fertility
HORMONAL THERAPY
The primary treatment for patients with Klinefelter syndrome is testosterone-based hormone treatment. The aim is to raise the low levels present in the blood.
Testosteronic hormone therapy begins at the time of puberty and, in some cases, lasts a lifetime.
The table illustrates the main features of hormonal treatment.
- Strengthen the musculature of the body
- Increase the growth of facial, pubic and armpit hair
- Increase libido
- Increase the size of the testicles
- Protect from osteporosis
- Reduce blood cholesterol levels
- On the sterility of patients
- On the development of the breasts (gynecomastia)
TREATMENT OF GYNECOMASTIA
Abnormal development of the breasts very often creates depression and a sense of embarrassment in patients. Therefore, the possibility exists to undergo surgery to reduce the volume of the breast. In fact, fat and glandular tissue is eliminated. It is a "somewhat invasive operation.
TREATMENT OF STERILITY € (INFERTILITY €)
The patient with Klinefelter syndrome, who wishes to have children, should consult a geneticist and a male infertility specialist.
The first is called to assess whether there is the possibility of a hereditary transmission of the disease. The second has the task of investigating the patient's ability to spermatogenesis, in order to understand if there is a concrete possibility of conception.
If even a minimal amount of spermatozoa is mature and capable of fertilizing an egg (or oocyte), one can proceed to:
- In Vitro Fertilization (IVF)
- Intracytoplasmic Sperm Injection (ICSI) into the oocyte
PSYCHOLOGICAL TREATMENT
The psychological aspect is very important. Testosterone administration, surgical breast reduction and possible fertility improve the self-esteem of patients with Klinefelter syndrome. They, in fact, manage to overcome the sense of exclusion from an active social life and relationship, which is, however, common to their peers.
OTHER TREATMENTS
Some patients experience symptoms even before puberty. The table shows the possible countermeasures to be adopted in the presence of some of these disturbances.
Prognosis
Hormone treatment is essential to improve the quality of life of patients with Klinefelter syndrome. In fact, in addition to overcoming the physical deficits due to the disease, they also improve their integration into social life.
The prognosis becomes worse, however, for those who are not treated promptly or who have mental retardation. In particular, in untreated subjects, azoospermia, infertility and small testes are irreversible conditions.