Generality
Crouzon's syndrome is a rare genetic disease, which determines the presence of craniosynostosis and other rather peculiar facial anomalies.
Its appearance is caused by certain alterations in the DNA that constitutes the FGFR2 and FGFR3 genes; these genetic elements are involved in the bone maturation process during embryonic development.

Therapy consists of a series of surgical interventions, aimed at resolving the most important and most dangerous symptoms.
Currently, the prognosis tends to be very often positive.
Review of genetics
Before proceeding with the description of Crouzon syndrome, it is useful to review some fundamental concepts of genetics.
What is DNA? It is the genetic patrimony, in which the somatic traits, the predispositions, the physical qualities, the character, etc. of a living organism are written. It is contained in all the cells of the body having a nucleus, as lies within this.
What are chromosomes? According to the definition, chromosomes are the structural units in which DNA is organized. Human cells contain, in their nucleus, 23 pairs of homologous chromosomes (22 of the autosomal non-sexual type and one pair of the sexual type); each pair is different from another, as it contains a specific gene sequence.
What are genes? They are short stretches, or sequences, of DNA with a fundamental biological meaning: from them, in fact, proteins, or biological molecules fundamental for life, derive. In the genes, there is "written" part of who we are and who we will become.
Each gene is present in two versions, the alleles: one allele is of maternal origin, therefore transmitted by the mother; the other allele is of paternal origin, therefore transmitted by the father.
What is a genetic mutation? It is a mistake within the DNA sequence, which forms a gene. Because of this error, the resulting protein is either defective or completely absent. In both cases, the effects can be deleterious both for the life of the cell, in which the mutation occurs, and for that of the organism as a whole. Congenital diseases and neoplasms (ie tumors) belong to one or more genetic mutations.
What is Crouzon's syndrome
Crouzon syndrome is a rare genetic condition characterized by craniosynostosis and an "unnatural development of certain facial elements, including the eyes, nose, jaw and jaw."
It is a congenital disease, the typical characteristics of which can be evident already during the first moments of life.
MEANING OF CRANIOSINOSTOSI
Craniosynostosis is the term by which doctors refer to the premature fusion of one or more cranial sutures.

From the site: thecraniofacialcenter.com
Cranial sutures are the fibrous joints that join the bones of the cranial vault together (i.e. the frontal, temporal, parietal and occipital bones).
Under normal conditions, the fusion of the cranial sutures occurs in the post-natal period (some processes even end at the age of 20). This long process of fusion allows the brain to grow and develop adequately.
If, as in the case of craniosynostoses, the fusion takes place too early - therefore during prenatal, perinatal * or early childhood life - the brain elements (brain, cerebellum and brainstem) and some sense organs (eyes in particular) undergo an "alteration of shape and growth.
* The perinatal term refers to the period of life that goes from the 27th week of gestation to the first 28 days following childbirth.
ORIGIN OF THE NAME
Crouzon syndrome owes its name to the French doctor Octave Crouzon, who has the merit of having first described its main clinical characteristics.
Crouzon lived between the late 1800s and early 1900s, exactly from 1874 to 1938. Initially, to define the syndrome that later took his name, he used the term craniofacial dysostosis.
Causes
Crouzon syndrome occurs as a result of a mutation in the FGFR2 gene, located on chromosome 10, or the FGFR3 gene, located on chromosome 4.
FGFR is the English acronym for Fibroblast Growth Factor Receptor, which translated into Italian is: Receptor for the Fibroblast Growth Factor.
The functional role of the FGFR2 and FGFR3 genes is each to produce a receptor protein, which in turn has the task of regulating the maturation and embryonic development of bone tissue.
According to the theories of the researchers, the mutations in FGFR2 and FGFR3 would hyper-stimulate these same genes, which, once more active, would induce an early maturation of some bone tissues, including those making up the skull.
GENETICS
The genetic mutations responsible for Crouzon syndrome can be hereditary or can arise spontaneously after conception.
In the first case, the morbid condition - which doctors also refer to as hereditary Crouzon syndrome - has all the characteristics of an autosomal dominant genetic disease (or inherited dominant disease). For a novice reader of genetics, this means that:
- The disease and its symptoms also occur in the presence of only one mutated gene allele (it does not matter if it comes from the mother or the father), as the latter is dominant over the healthy one.
- A parent carrying the mutation is enough to have the disease in part of the progeny.
- The probability that a sick child will be born, from a couple where only one of the two components carries the mutation, is 50%.
In the second case, however, the morbid condition - which experts indicate with the terminology of non-hereditary Crouzon syndrome - is the result of an anomalous sporadic event, which alters the DNA during the embryonic growth of the fetus.
Summary of the meaning of the terms hereditary, autosomal and dominant
- Hereditary: it means that the parents transmit the genetic alteration responsible for the disease to the offspring (ie to the children).
- Autosomal: it means that the mutation responsible for the disease resides in a non-sex chromosome, therefore autosomal.
- Dominant: means that the disease causes symptoms and signs even when only one allele of the responsible gene is mutated. In simpler terms, it is as if the allele with the mutation had more power than the healthy allele.
EPIDEMIOLOGY
According to some estimates of the incidence rate of Crouzon syndrome, about one in 60,000 children would be born with this rare condition.
Crouzon syndrome accounts for 4.5% of craniosynostosis cases.
Symptoms and Complications
Patients with Crouzon syndrome have a very specific symptom picture, which usually consists of:
- Problems related to craniosynostosis, including:
-
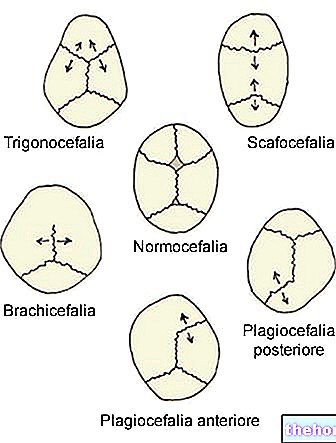
From https://en.wikipedia.org/wiki/Plagiocephaly Brachycephaly, which is the squeezing of the back of the head. Premature fusion of the coronal cranial sutures follows (coronal craniosynostosis).
If left untreated, it can affect brain growth and development of cognitive abilities.
They represent an "alternative to brachycephaly: trigonocephaly (fusion of the metopic suture), dolichocephaly (fusion of the sagittal suture) and plagiocephaly (fusion of the coronal sutures). - Exophthalmos, which is the term for the protrusion of the eyeballs. It could imply the presence of vision problems.
- Ocular hypertelorism, that is, eyes that are exaggeratedly distant from each other. With exophthalmos, it can make vision problems worse.
- Deformed nose, generally in the shape of a beak. If severe or not treated surgically, this abnormality can lead to breathing problems or the same symptoms as obstructive sleep apnea syndrome.
- Increased intracranial pressure. It is also known as intracranial hypertension. Its presence is explained by the fact that the brain structures do not have the right space to grow.
Usually found in mid-late childhood, intracranial hypertension is a potential cause of headache, vomiting and eye pain. - Hydrocephalus, which is the result of an increase in the cerebrospinal fluid contained in the subarachnoid space and in the cerebral ventricles.
- Arnold-Chiari malformation (or Arnold-Chiari syndrome). It is a deformity located at the base of the skull.
* Hydrocephalus and Arnold-Chiari malformation are generally two complications that arise in the absence of adequate treatments. - Abnormalities in the mandible and maxilla.
The first has smaller dimensions than normal, while the second tends to protrude outwards. All this changes the shape of the palate and the dental scaffold (absence of some teeth, etc.), with repercussions (sometimes even serious) on phonation and on the chewing.
Some patients are born with cleft lip (cleft lip) or cleft palate.
- Hearing problems.
55% of patients with Crouzon syndrome are born without the ear canals or with major abnormalities in them. This results in an absent or greatly reduced acoustic capacity.
Some subjects develop a set of hearing problems in adulthood, attributable to the typical clinical picture of Ménière's syndrome.
- Joint problems in the neck.
They concern 30% of Crouzon syndrome cases.
- Skin anomalies.
Patients with mutated FGFR3-supported Crouzon syndrome present acanthosis nigricans, a dermatosis characterized by an increase in thickness (hyperkeratosis) and darkening (hyperpigmentation) of the skin.

Two other anatomical anomalies associated (albeit rarely) with Crouzon syndrome
- Patent arterial duct
- Coarctation of the aorta
CROUZON SYNDROME AND IQ
Thanks also to the current possibilities of treating craniosynostosis, today 97% of patients with Crouzon syndrome have "normal intelligence."
Diagnosis
An experienced pediatrician may be able to diagnose Crouzon syndrome by means of the physical examination alone.
In the presence of any doubt or perplexity, the following are fundamental to arrive at a precise conclusion:
- Radiological images, provided by X-rays or CT scans of the head
- A genetic test, aimed at looking for any DNA mutations.
OBJECTIVE EXAMINATION
The physical examination consists in an accurate analysis of the head and the anomalies present on it.
Cranial deformities, induced by craniosynostosis (for example brachycephaly), are among the most characteristic clinical signs of Crouzon syndrome and on which the doctor bases part of his diagnostic conclusions.
RADIOLOGICAL EXAMINATIONS
X-rays and CT scans of the head show which cranial sutures have fused prematurely.
The craniosynostosis that characterizes Crouzon's syndrome affects the coronal sutures, therefore a found fusion at the level of the latter is a very often decisive information for diagnostic purposes.
GENETIC EXAMINATION
In addition to showing if the DNA has mutations, genetic testing helps identify the exact gene that causes Crouzon syndrome, whether FGFR2 or FGFR3.
Treatment
Today, Crouzon syndrome carriers can count on various treatments, depending on the severity of the condition and the symptoms.
In fact, doctors have ensured:
- Surgery for the resolution of craniosynostosis and its symptoms.
- Acoustic aids, in case of hearing problems.
- Therapies for the improvement of language skills.
- Surgical therapies for the improvement of anomalies in the maxilla and mandible.
- A surgery, known as a tracheostomy, to resolve breathing problems.
Please note: Crouzon's syndrome is a morbid condition that derives from a "genetic alteration of the DNA that is impossible to cure. So, in fact, doctors treat the disease only from a symptomatic point of view.
SURGERY FOR CRANIOSYNOSTOSIS
The therapeutic objectives of the surgical operation are two:
- Provide the brain structures and eyes with the space they need to develop and function at their best.
- Give the head a normal shape, then solve the problem of brachycephaly.
Surgeons have the possibility to perform the operation in two different ways (or approaches): through a "traditional surgery operation - also called" open "- or through an" endoscopic surgery operation.
The "open surgery" involves the "execution of a" incision on the head, through which the operating physician extracts the bone or the malformed cranial bones which must be remodeled. At the end of the remodeling, the surgeon reinserts the bone structures previously extracted and closes the incision with sutures.
The endoscopic surgery, on the other hand, involves the use of an endoscope and the practice of a very small incision on the head, through which the operating doctor inserts the endoscope itself.
The endoscope is in fact a thin and flexible tube, fitted with a fiber optic camera (at the end inserted into the skull) and connected to a monitor. Through this particular instrument and the images it projects on the monitor, the surgeon is able to separate the fusing cranial sutures prematurely, with remarkable precision and without resorting to skin incisions and bone extractions.
According to experts, the best time to perform the surgery is during very early childhood (first 12 months of life), as the bones are more easily molded.
However, it should be remembered that the younger the patient, the higher the risk of a recurrence of the same cranial sutures (recurrence). In case of recurrence, the surgery must be repeated.
According to some statistical research, 10-20% of very young subjects, undergoing craniosynostosis surgery, need to undergo a second operation, due to a relapse.
TREATMENT OF ACOUSTIC PROBLEMS
In addition to prescribing the use of hearing aids, doctors also recommend periodic auditory checks, as this is the best way to prevent any worsening of existing problems.
SURGICAL THERAPIES FOR JAW AND JAW ANOMALIES
The treatment of maxillary and mandibular anomalies includes surgery for the realignment of the maxilla and / or mandible, some dental treatments for the arrangement of the dental arches and the operation for the resolution of the cleft lip and / or cleft palate.
TRACHEOSTOMY
The tracheostomy is the surgical operation through which the doctor creates, at the level of the neck (where the trachea passes), a passageway for the air destined for the lungs. This allows those who undergo this surgery to breathe again and correctly.
To convey the air into the lungs, you need a small tube, called a transcheostomy tube, which is the right size for insertion into the trachea.
Prognosis
In general, the prognosis depends on the severity of the craniosynostosis: if the latter is treatable with good results, patients with Crouzon syndrome can enjoy an almost normal life.