This disease owes its name to the American endocrinologist who discovered it: Frederic Crosby Bartter. The annual incidence has been estimated at 1 / 830,000.
There are several variants of Bartter's syndrome whose transmission, although still autosomal, can vary from recessive to dominant depending on the case.
If not promptly diagnosed and treated, Bartter's syndrome can severely compromise the patient's development, growth and quality of life. Furthermore, in particularly severe cases, life expectancy is considerably reduced.
Please Note
Bartter syndrome should NOT be confused with Schwartz-Bartter syndrome, a disease characterized by "impaired secretion of antiduiretic hormone (ADH), also known as the syndrome of inappropriate ADH secretion (SIADH).
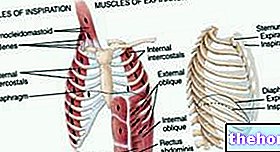
.which occurs at the level of the loop of Henle is attributable to an "alteration of the synthesis of some channel / transporter receptors (particular proteins that transport ions of different nature) located in this" area of the kidney. This phenomenon is caused by a series of genetic mutations affecting the genes encoding the aforementioned particular proteins.
The different variants of Bartter's syndrome are distinguished according to the affected gene. More detailed information on this can be found in the following chapter.
.
The following table will therefore show the different variants of the syndrome, the mutated genes involved, the proteins (channel receptors / transporters) for which they encode and the clinical presentation of the variant in question.
Variant
Mutated gene
Channel / Transporter Involved
Clinical Presentation
Bartter syndrome type I
Gene SLC12A1
NKCC2 (sodium-potassium-chlorine cotransporter or Na + / K + / 2Cl-)
Prenatal (or infantile) Bartter syndrome
Bartter syndrome type II
Gene KCNJ1
ROMK (potassium channel of the external medulla of the kidney)
Prenatal (or infantile) Bartter syndrome
Bartter syndrome type III
Gene CLNKb
CLCNKb (Kb type chlorine channel)
Classic Bartter syndrome
Bartter syndrome type IV or IV A
Gene BSND
Barttina (beta subunit of Ka and Kb type chlorine channels)
Prenatal (or infantile) Bartter syndrome and sensorineural deafness
Bartter syndrome type IV B
CLCNKa and CLCNKb genes
CLCNKa (Ka type chlorine channel) and CLCNKb
Prenatal (or infantile) Bartter syndrome and sensorineural deafness
Type V Bartter syndrome
CASR gene
CaSR (calcium sensitive receptor)
Bartter syndrome with hypocalcemia
As can be seen from the table, despite the presence of five genetic variants, it is not possible to distinguish as many clinical forms; in fact, only four are distinguished: prenatal or infantile Bartter syndrome (type I and II), classic Bartter syndrome (type III), prenatal or infantile Bartter syndrome associated with sensorineural deafness (type IV A and IV B; some sources, however, they group these variants together with type I and II) and, finally, Bartter syndrome with hypocalcemia (type V).
Did you know that ...
Given the existence of a variant IV (or IV A) and a variant IV B of Bartter syndrome, some sources consider, overall, six variants of Bartter syndrome.Other sources, however, consider variant IV B as a subtype of variant IV and, for this reason, contemplate the existence of only five genetic variants of Bartter's syndrome.
The variants of types I, II, III, IV and IV B are autosomal recessive diseases, which means that to manifest the syndrome, the individual must possess both mutated alleles inheriting them from the parents who, therefore, will be healthy carriers. Variant V of the syndrome, on the other hand, is an autosomal dominant transmission disease, which means that in order to manifest the symptoms, it is sufficient for the patient to possess a single mutated allele which, therefore, can be inherited even by only one (also sick) of the two parents.
Bartter's pseudo-syndrome
Bartter's pseudo-syndrome is a condition characterized by symptoms similar to those induced by Bartter's syndrome but whose cause is to be found in the abuse of diuretic drugs such as furosemide.
Gitelman syndrome
This syndrome is caused by a localized mutation on the SLC12A3 gene that codes for the sodium-chlorine cotransporter (NCC). Due to this mutation - transmitted in an autosomal recessive manner - the patient undergoes an impairment of the reabsorption of sodium, chlorine and potassium at the level of the distal convoluted tubule, unlike Bartter's syndrome in which the impairment of resorption is localized in the " However, Gitelman's syndrome can give rise to a symptomatology similar to that of Bartter's syndrome, therefore, in clinical practice, it can sometimes be difficult to distinguish the two diseases.
, hypochloremia and metabolic alkalosis which can be associated with hyperreninemia (high blood renin) and hyperaldosteronism. Clearly, all these conditions can, in turn, give rise to a series of symptoms capable of compromising the patient's quality of life (for example, nausea, vomiting, dizziness, weakness, headache, hypotension, etc.).
In addition to what has been said so far, each variant can give rise to specific manifestations and symptoms closely related to the mutated gene and to the consequent involvement of the channel or cotransporter for which this gene encodes. Therefore, the typical symptoms and manifestations associated with each of the five different forms of Bartter's syndrome will be briefly described below.
Bartter syndrome type I
In Bartter syndrome type I the mutations affect the gene coding for the sodium-potassium-chlorine cotransporter present on the loop of Henle. Due to the compromised reabsorption, hypovolemia occurs due to loss of salts. At the same time, since the reabsorption of calcium is also linked to the activity of the aforementioned cotransporter, we are witnessing the onset of hypercalciuria. All this can lead to the onset of nephrocalcinosis. It is also possible to experience hypermagnesuria. In the prenatal period, polyhydramnios secondary to fetal polyuria may develop.
Bartter syndrome type II
Bartter syndrome type II is caused by a mutation in the gene that codes for the potassium channel of the adrenal medulla. Manifestations and symptoms are similar to those of variant I and also in this case one can encounter polyhydramnios secondary to fetal polyuria. However, at an early stage, the infant may experience transient hyperkalaemic metabolic acidosis. This condition then evolves towards the characteristic clinical picture of Bartter's syndrome.
Bartter syndrome type III
Also known as classical Bartter syndrome, variant III of the disease is caused by mutations in the gene coding for the Kb type chlorine channel. Since the Ka type chlorine channels are preserved in this form, symptoms tend to to be lighter, although still present. There is generally no nephrocalcinosis.
Bartter syndrome type IV and IV B
In both types of variant IV there is the involvement of genes involved in the correct synthesis of the Ka and Kb chlorine channels. Since both channels are compromised, the symptoms tend to be more severe than for variant III of the syndrome. . Infants may initially show a clinical picture that mimics hypoaldosteronism but which then evolves towards hypokalaemic metabolic alkalosis when the body tries to compensate for the lack of activity of the aforementioned calcium channels. Characteristic of variants IV and IV B of Bartter's syndrome is the appearance of sensorineural deafness.
Type V Bartter syndrome
Variant V of Bartter's syndrome is caused by a mutation affecting the gene coding for the calcium-sensitive receptor, involved in the inhibition of the reabsorption of water and various ions, such as calcium, potassium and sodium. receptor leads to the appearance of hypocalcemia and consequent hypercalciuria associated with the characteristic symptoms of Bartter's syndrome.
Did you know that ...
Variants I, II, IV and IV B of Bartter syndrome - as well as with the name of prenatal Bartter syndrome - are sometimes also referred to as hypeprostaglandin E2 syndrome, since they are characterized by an increase in plasma levels of this prostaglandin.
- aimed at identifying the presence and concentration of electrolytes (sodium, potassium, chloride, magnesium, bicarbonate, calcium) and specific substances (renin and aldosterone) in plasma and / or urine.The definitive diagnosis is however possible only with the execution of specific genetic tests.
The differential diagnosis, on the other hand, must be placed against Bartter's pseudo-syndrome, Gitelman's syndrome, cystic fibrosis and celiac disease.
In cases where there is a certain risk (for example, parents with healthy and / or sick carriers) that the newborn may manifest the disease, prenatal diagnosis is also possible.
from:
- Supplements of mineral salts (in particular but not exclusively, potassium) in order to compensate for the lack of reabsorption;
- Non-steroidal anti-inflammatory drugs (NSAIDs) such as, for example, indomethacin. These drugs are administered with the aim of decreasing excessively high levels of prostaglandin E2;
- Potassium-sparing diuretics (given to reduce potassium excretion in the urine).
In the most serious cases and / or in stressful conditions (onset of other diseases, surgical interventions, etc.), the replenishment of potassium and other mineral salts can be carried out intravenously, of course, a similar operation must be carried out by health personnel specialized.





-cos-cause-e-terapia.jpg)