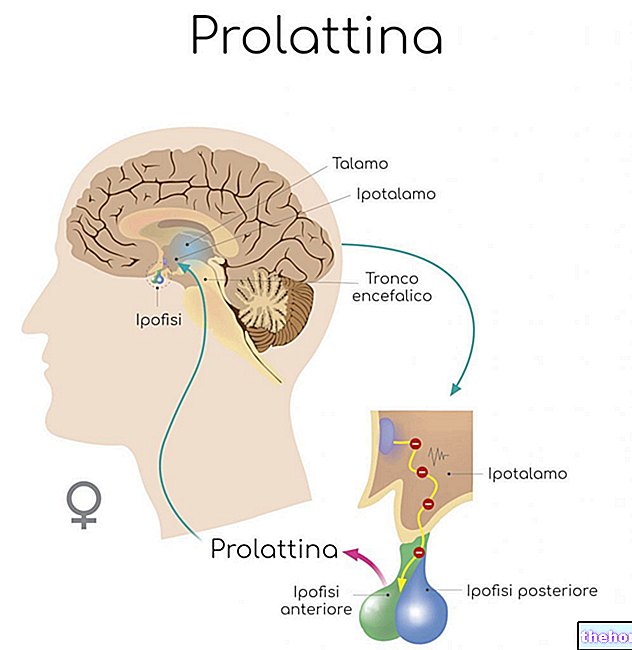
«Introduction: the hypothalamus-pituitary axis
Causes
Increases in prolactin levels (hyperprolactinaemia) can occur:
For causes physiological: pregnancy, puerperium, stress, exercise, sleep, protein-rich meals, breastfeeding, sexual activity;
For some use medications: tricyclic antidepressants, antiepileptics, antihypertensives, antiemetics (against nausea and vomiting), antihistamines, cocaine, sometimes birth control pills, metoclopramide-sulpiride, veralipride;
Unknown causes (idiopathic);
Causes pathological: pituitary adenoma (benign prolactin-secreting tumor, also called prolactinoma), non-secreting pituitary adenomas, acromegaly, empty sella syndrome, Cushing, meningiomas (malignant tumors of the meninges), dysterminoma (testicular cancer), other tumors, sarcoidosis;
Causes neurological: Herpes Zoster chest wall injuries, spinal cord injuries;
Other causes of hyperprolactinemia: hypothyroidism, renal failure, liver cirrhosis, adrenal gland failure.
Aftermath
Hyperprolactinemia determines various alterations in reproductive function, up to the lack of ovulation in women. This is because the hypothalamus-pituitary-ovary axis is sensitive even to small elevations in circulating prolactin levels. In fact, an altered secretion of prolactin is very frequently associated with amenorrhea (lack of menstruation) or other menstrual disorders. It is estimated that about 15-30% of secondary amenorrhoea, ie not due to ovarian disorders, is due to hyperprolactinemia. Hyperprolactinemic amenorrhea is characterized by the elevation of prolactin levels with a value greater than 25 nanograms per milliliter, visible with a simple blood test. In about 30-50% of cases, hyperprolactinemic amenorrhea is accompanied by galactorrhea, ie the spontaneous release from the nipple of a milky secretion outside the lactation period. In this case, you will have the so-called galactoreal amenorrhea syndrome.
In 50% of cases, amenorrhea is preceded by menstrual irregularities of various types, such as oligomenorrhea (delaying cycles), hypomenorrhea (scanty menstruation), menorrhagia (menstruation that is too long), metrorrhagia (intermenstrual bleeding, generally post-ovulatory, also called spotting). Other symptoms related to hyperprolactinemia, more rare, are headache and visual disturbances, when the tumor expands.
Prolactinecerning pituitary adenomas
They deserve a separate discussion with respect to all other causes of hyperprolactinemia, since they are the most frequent functional (ie prolactin-producing) benign tumors of the pituitary. They represent 60-70% of all pituitary adenomas. Typically these tumors are discovered in women of reproductive age who present more or less suddenly menstrual disturbances referable to a situation characterized by an increase in circulating levels of prolactin. The evolution of these tumors is usually slow and gradual, but in isolated cases a rapid increase in the levels is also possible. their size. Most of them are microprolactinomas, that is, smaller than 10 millimeters in diameter. Untreated, they seem to undergo a progressive reduction over time, or in any case tend to remain stable. Furthermore, they frequently undergo spontaneous partial necrosis (destruction). The age distribution in which they can occur varies from 2 to 84 years, with a peak incidence around 60 years. The frequency between the two sexes is similar; however, clinical manifestations, especially changes in reproductive function, are more frequent in women.
Diagnosis
From the diagnostic point of view, the main problem consists in the differentiation of hyperprolactinemias tumors from those non-cancerous (functional). Today it is quite common in the belief that there is no clear limit between these two forms, both because some particularly small microadenomas can escape the current means of investigation, and because it is possible that the hyperstimulated pituitary cells pass through different stages of activity, from simple hyperfunction to hyperplasia (multiplication) up to producing frank adenomas (uncontrolled multiplication), more or less tending to compression of the surrounding tissues.
In all cases in which the "existence of" an alteration in the production of prolactin is suspected (amenorrhea, with or without galactorrhea; failure to ovulate; intermenstrual spotting, etc.) it is first of all necessary to measure the plasma prolactin with a simple blood test. Once its high value has been ascertained, more dosages (two or three) must be carried out over the course of 24 hours and for several days, in order to eliminate errors related to variations during the day and the withdrawal stress. An alternative and more practical method, similar to the previous one, can be that of the three dosages to be carried out in the "span of an hour and a half, one half an hour apart", interspersed with the administration of a physiological solution via a drip.
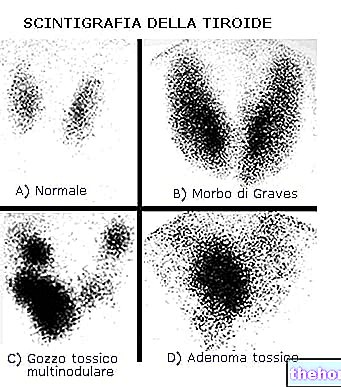
In the presence of persistently high values, higher than 60 nanograms per milliliter, in all three leads, after having excluded the existence of hypothyroidism with the plasma dosage of the thyroid hormones T3 and T4 and TSH, we will move towards an adenoma of the pituitary; therefore a will be performed CT (computed tomography) or one TMR (magnetic resonance tomography) with contrast medium of the sellaturchica, which is the anatomical structure at the base of the skull in which the pituitary is contained. They allow to appreciate the presence of microadenomas and adenomas of the pituitary gland and their possible extension to the surrounding structures, especially to the optic chiasm , a structure formed by the nerve extensions of the optic nerve that passes immediately above the saddle. If the tumor compresses the chiasm, the patient could have visual field disturbances which, even if asymptomatic, can be highlighted with a test called campimetry, generally complementary to CT and TMR. Above all, it allows to evaluate the possible expansion of the tumor; therefore, while it does not seem absolutely necessary in the presence of a microadenoma, it is extremely useful and necessary in the surveillance of the evolution of macroadenomas.
Other articles on "Hyperprolactinemia"
- Treatment of hyperprolactinemia
- Hyperprolactinemia - Drugs for the treatment of Hyperprolactinemia