«Hyperprolactinemia
Therapy
Normalization of plasma prolactin levels should be proposed. In some cases this objective can be easily achieved, for example in hypothyroidism, with an appropriate replacement treatment with thyroid hormones and, in the forms of hyperprolactinemia due to the use of drugs, by interrupting the administration of the same.
On the other hand, the therapeutic problem appears more complex in the forms of microadenoma and in the so-called "idiopathic" forms which, however, in most cases are caused by microadenomas whose existence is not demonstrable with current diagnostic means.
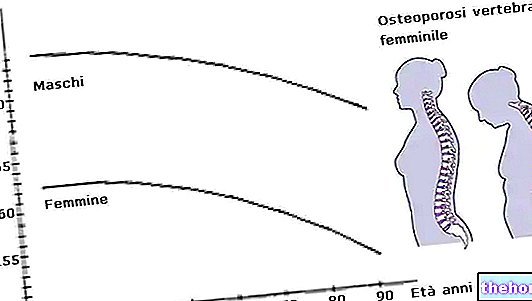
There is still no agreement on the need for treatment, since many studies show that their long-term evolution is towards stabilization and not towards growth. However, it is advisable to lower the hormone levels if hyperprolactinemia is associated to a series of disorders of reproductive function (menstrual irregularities, failure to ovulate, etc.), of sexual life (frigidity, pain felt during sexual activity) and of bone mineralization (osteoporosis). Therapy, in these cases, can be medical, surgical or radiotherapy.
There medical therapy it represents the first choice both in the forms of hyperprolactinemia due to pituitary micro and macroadenomas, and in the idiopathic forms. Medical therapy uses a series of drugs with a stimulating action on receptors that are activated by dopamine (a hormone in the brain). The most widely used hypoprolactinemizing drugs are:
cabergoline (trade name Dostinex) and bromocriptine (Parlodel). Others are lisuride, lergotrile, pergolide, metergoline and dihydroergocriptine.
The drugs cause a rapid reduction in prolactin values and consequent remission of clinical symptoms in 95% of cases. They also lead to a reduction in the volume of macroadenomas in 60-70% of cases and to the complete disappearance of the lesion in 10-15% of cases of microadenoma. The wide choice of these dopaminergic drugs makes it possible to overcome intolerance phenomena that can occur with a drug by replacing it with another.
Carbegoline and bromocriptine inhibit the synthesis and release of prolactin by acting both at the hypothalamic and at the pituitary level. Furthermore, they are able to reduce the size of prolactin-secreting pituitary adenomas. Carbegoline has a very long duration of action, so a single dose per week is sufficient. Bromocriptine, on the other hand, must be administered several times during the same day. The side effects of carbegoline are also considerably less than those of bromocriptine. When present, they occur from the first administration and consist of a drop in blood pressure, especially during standing, nausea and vomiting, neuropsychiatric disorders, sometimes hallucinations. To minimize the possibility of experiencing these effects it is necessary to start treatment with Dostinex at reduced doses: half a 0.5 milligram tablet every week for two weeks until the dosage of 1-2 milligrams per week is reached.
Discontinuation of treatment is usually followed by resumption of tumor growth, so therapy must be continued indefinitely.
In some cases of physiological hyperprolactinemia (not due to pituitary adenomas), especially those caused by stress and sleep, in women who do not wish to become pregnant, it is preferable to administer an estrogen-progestogen contraceptive pill to regulate the menstrual cycle, since its side effects are usually lower than those given by the dopaminergic drugs just described.
There surgical therapy consists in the surgical removal of prolactin-secreting pituitary adenomas. It is carried out transphenoidally and an endoscope is used (a small flexible tube equipped with a camera at its apex) which is introduced into one of the two nostrils of the patient, previously anesthetized. The camera is connected to a digital video system. The endoscope must reach the spheroidal sense, and from there to the sella turcica, where the adenoma will be identified and removed. Surgery should be indicated only in case of intolerance or more or less total resistance to medical treatment, which occurs in one third of cases of microadenomas.
There radiotherapy today it has a completely secondary role and exceptional indications. Its use is limited to the treatment of surgical failures.
Monitoring of pituitary adenomas
Given the slow growth of the tumor, patients with microadenoma should be checked once a year with measurement of plasma prolactin levels and with a CT of the sella turcica; in the absence of growth, CT can be performed every 2-3 years. More sophisticated and more frequent checks are instead necessary in the presence of an increase in prolactin levels, the onset of headache or visual disturbances, or changes in CT. Patients with macroadenoma require closer surveillance, yearly or better still every six months, associating the exams indicated above with a magnetic resonance imaging (MRI) or a magnetic resonance tomography (TRM).
Other articles on "Treatment of" Hyperprolactinemia "
- Hyperprolactinemia
- Hyperprolactinemia - Drugs for the treatment of Hyperprolactinemia