Generality
Ventricular fibrillation is an arrhythmia characterized by rapid, ineffective and irregular contractions of the ventricles. This results in severe impairment of cardiac output, such that ventricular fibrillation is considered a leading cause of cardiac arrest or sudden cardiac death.

The symptoms of atrial fibrillation (palpitations, chest pain, cyanosis, dyspnea and loss of consciousness) arise very quickly, so much so that the therapeutic intervention, to have a success rate, must be timely. Action must be taken immediately if the patient is to be saved. Emergency treatment mainly consists of cardioversion (or defibrillation). However, alternative therapeutic approaches should not be forgotten, such as cardiopulmonary resuscitation, through cardiac massage, and the administration of certain drugs. As for the diagnostic tests (electrocardiogram, echocardiogram and chest X-ray), ventricular fibrillation has such a rapid course that it does not allow time for an accurate investigation of the causes of the disorder.
N.B .: to understand some concepts illustrated in the article, it is necessary to know the basics of anatomy and physiology of the heart illustrated in the general article on cardiac arrhythmias.
What is ventricular fibrillation
Ventricular fibrillation is an alteration of the heartbeat at the level of the ventricles, which contract rapidly and in a disorderly manner. The heartbeat and contractions change accordingly, taking on the following characteristics:
- Increased frequency and speed.
- Irregularity and lack of coordination.
- Variable intensity.
- Mechanical ineffectiveness.
The mechanical ineffectiveness arises because the overlapping of numerous contractile impulses does not allow the muscles of the ventricle to respond effectively. In other words, the stimuli of contraction, at the time of the systole phase, are so numerous that they do not translate into as many effective and adequate responses. This is due to the fact that the myocardial cells, once contracted, need a certain time interval to become receptive again (refractory time). This time interval, identifiable with the diastole phase (ie the relaxation of the myocardium), is respected when the heart beats regularly; vice versa, when the rhythm increases dramatically, the time between one impulse and the other is so short that it does not determine any concrete cellular response. Furthermore, the desynchronization of the contraction of the various myocardial fibers makes it impossible to develop a ventricular pressure capable of opening the valves. aortic and pulmonary and to produce systolic output.
All these changes imposed on the heartbeat compromise cardiac output, operated by the contraction of the ventricle. Cardiac output corresponds to the flow of oxygenated blood that is pumped into the circulation towards the organs and tissues of the human body (including the heart, which receives arterial blood from the coronary arteries that originate in the first part of the aorta). blood is insufficient, oxygenation becomes deficient. Consequently, a condition of anoxia is created such that even the heart is gradually less and less oxygenated and able to perform its contractile function effectively.The final outcome of this situation is the death of the heart, from acute anoxia, and the consequent arrest of blood circulation. What makes these events even more dramatic is their rapid onset and progression.
Ventricular fibrillation, therefore, is an "alteration of the rhythm with a rapid and inauspicious course, which places it among the most decisive arrhythmias in causing death from cardiac arrest or sudden cardiac death.
80-85% of cardiac arrest deaths are caused by ventricular fibrillation. It has been estimated that, in the Western world, it affects 1 person in 1,000 per year. Men are more affected than women: the ratio is 3: 1.
The incidence of ventricular fibrillation is higher in those 50-70 year olds with pre-existing cardiac ischaemia. However, as will be seen shortly, ventricular fibrillation can also arise in the absence of ischemic heart disease, such as, for example, in some juvenile and congenital syndromes.
Causes
The main causes of ventricular fibrillation are:
- Hypoxia, due to:
- Coronary heart disease.
- Cardiac ischemia.
- Myocarditis.
- Valvulopathies
- Metabolic acidosis.
- Hypokalemia.
- Hyperkalemia.
- Hypocalcemia.
- Hypomagnesemia.
- Trauma to the heart, accidental or surgical.
- Electric discharges:
- Alternating currents between 20 and 150 mA.
- Continuous currents between 80 and 600 mA.
- Incorrect or improper pharmacological treatments, based on:
- Tricyclic antidepressants.
- Antiarrhythmics.
- Hyperthyroidism.
- Wolff-Parkinson-White syndrome.
- Brugada syndrome.
- Gas poisoning:
- Carbon monoxide (CO).
- Cyclopropane.
- Narcotic poisoning:
- Cocaine.
As you can see, the causes are numerous and each has specific characteristics. Treating them in detail is not the purpose of this article. However, a brief parenthesis will be devoted to why certain phenomena, such as hypoxia, electrolyte imbalances, improper intake of drugs, electrical discharges, etc., determine the onset of ventricular fibrillation. create an ionic / electrolytic imbalance across the membranes that make up the cells of the myocardium; imbalance that compromises the passage of the contractile impulse. The importance of the correct distribution of charged ions (positive or negative), such as calcium, potassium, magnesium, etc., is fundamental for transmitting the contraction signal, which is an electrical signal. If this equilibrium fails , the cells no longer function adequately and, in this specific case, contract with very high frequencies and in an irregular way.
Finally, the cases of ventricular fibrillation in healthy individuals should not be forgotten. We speak of idiopathic ventricular fibrillation, as the causes are not known. The onset is paroxysmal in nature: therefore, it is sudden and spontaneous.
Symptoms
The typical symptoms of ventricular fibrillation arise very quickly and are consequential to each other. They are:
- Dyspnea.
- Loss of consciousness.
- Chest pain.
- Palpitation.
- Stopping of circulation
- Feeling of fatigue.
- Cyanosis.
Due to the seriousness of the situation that arises, the timeliness in identifying and understanding the symptoms is essential to save the life of the individual affected by ventricular fibrillation.
Diagnosis
In most cases, the rapidity with which the arrhythmic disorder evolves and the consequent need for immediate intervention do not leave the time to make a complete diagnosis. However, there may be some warning clinical signs due to an early stage myocardial infarction.
Possible diagnostic tests are:
- Electrocardiogram.
- Echocardiography.
- Chest X-ray.
- Coronary angiography.
Electrocardiogram. It is the instrumental examination indicated to evaluate the course of the electrical activity of the heart. In the case of ventricular fibrillation, the trace shows rapid and irregular oscillations, with an unmistakable appearance. They are the prelude to the arrest of all cardiac activity. If you come across a myocardial infarction in the initial phase, through ECG you can identify ventricular extrasystoles, which act as clinical warning signs of a ventricular fibrillation.
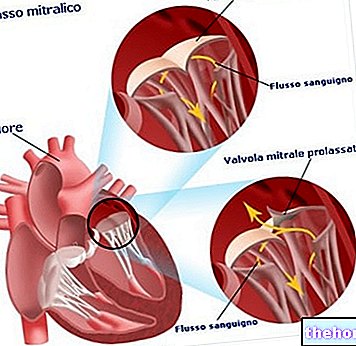
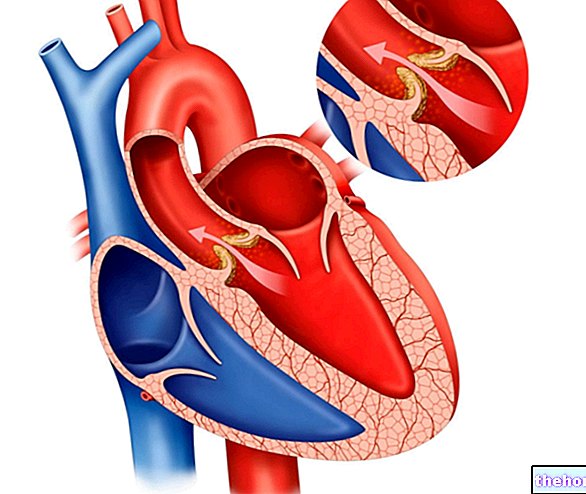
Echocardiography. By exploiting the emission of ultrasound, this non-invasive investigation shows the fundamental elements of the heart: atria, ventricles and valves. The evaluation of the heart allows to verify the presence of valvular anomalies or some other cardiac malformation.
Chest X-ray. It is a useful clinical investigation in providing information on the relationship between the heart and lungs. Pulmonary thrombosis, for example, may be associated with ventricular fibrillation events.
Coronary angiography. This is an invasive examination, aimed at assessing the health of the coronary system. An estimate of the level of coronary occlusion and a timely intervention, aimed at freeing the blocked vessels, can avoid the occurrence of ventricular fibrillation. A catheter is used that acts as a probe to trace the blocked site. Then we act to free this area. This is a delicate operation, because there is the risk of damaging the coronary vessels crossed by the catheter.
Therapy
The "therapeutic intervention must" be timely, as the evolution of the effects induced by the fibrillation is very rapid and dramatic. You have a few minutes, not more than five. In the event of cardiac arrest, various practices can be used:
- Cardioversion or defibrillation. Through a special device, an electric shock is infused to reset and restore the sinus heart rhythm. The shock is applied by means of two pads placed on the patient's chest. Current instruments are so efficient that they can detect the trend of ventricular fibrillation and, consequently, apply the right shock required. In other words, they self-adjust according to need. These are defined as semi-automatic or automatic defibrillators, which can be used even by non-medical personnel.
- Cardiopulmonary resuscitation (CPR). If you do not have a defibrillator and there is no time to get it, you have to act with CPR. It is a "cardiorespiratory action that replaces the natural one, practiced in order to pump blood into the circulation towards the lungs, brain and others. organs. It is carried out through the practice of mouth-to-mouth breathing and cardiac massage.
- Antiarrhythmic drugs. They serve as a support to the previous treatments just described. They have the function of maintaining normal heart rhythm even when it is possible to re-establish cardiac activity consonant with life. The most used drugs are amiodarone and lidocaine.
Prognosis
As has been said several times, the timeliness of intervention is essential to save the patient's life and safeguard the non-oxygenated organs at the time of cardiac arrest. Acting in time gives ample chance of survival.
The success of the surgery depends very much on the causes that triggered the ventricular fibrillation. If, for example, the patient's heart is suffering from severe heart disease, it may be more difficult to restore cardiac activity.