During diastole, the heart cavities - that is, the atria and ventricles - enlarge and fill with blood. During systole, however, the same cavities contract and empty of blood.
Thus described, the cardiac cycle - this is the name that takes the alternation between diastole and systole - appears very simple. In reality, however, the situation is slightly more complex than what has just been reported. Let's see why.
Systole can be divided into two moments: atrial systole, which corresponds to the contraction of only the atria and serves to transfer blood into the ventricles, and ventricular systole, which corresponds to the contraction of only the ventricles and serves to pump blood into the blood vessels.
Like systole, diastole also consists of two moments: the atrial diastole, which is the re-expansion of the atria before a new atrial systole, and the ventricular diastole, which is the re-expansion of the ventricles before a new ventricular systole.

Therefore, systole and diastole overlap over time, starting when one has already partially unfolded.
On the other hand, if they were two separate events - that first one occurs and then another occurs - the heart would not be able to guarantee the right amount of blood to the tissues that the latter need.
In other words, "lub" - which is considered, by convention, the first sound of the cardiac cycle - represents the beginning of the emptying of the atria and ventricles.
Turning to "dub", this is produced by the closing movement of the aortic and pulmonary valves at the end of systole and at the beginning of diastole (ventricular diastole to be exact).
It should be remembered that diastole is the phase of expansion and filling of the heart cavities, that is the moment in which the myocardium is released to receive the returning blood again.
In other words, "dub" - which, according to convention, consists of the second sound of the cardiac cycle - represents the beginning of the relaxation of the ventricles.
- which serve to regulate the flow of blood between the atria and the ventricles and between the ventricles and the blood vessels that branch off from the ventricles themselves. The correct closing and opening of the valves is essential to guarantee the unidirectionality of the blood flow.
Remembering that the heart can ideally be divided into two halves, the tricuspid valve and the pulmonary valve take place in the right half, while the mitral valve and the aortic valve are located in the left half.
More precisely…
The tricuspid valve is located between the right atrium and the right ventricle and is crossed by the oxygen-poor blood that has just supplied the organs and tissues of the body.
The pulmonary valve resides between the right ventricle and the pulmonary artery and is responsible for regulating the flow of blood to the lungs for oxygenation of red blood cells.
The mitral valve takes place between the left atrium and the left ventricle and is crossed by the blood coming out of the lungs and loaded with oxygen.
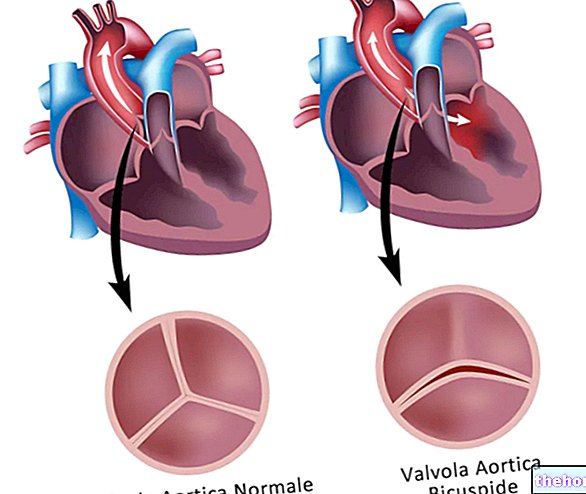
Finally, the aortic valve is located between the left ventricle and the aorta and has the fundamental function of making the blood flow towards the arterial system and towards the various organs of the body, for their oxygenation.
.
The heart is not on the left, but in a central position, between the two lungs.
The force with which the heart pumps blood into the circulation is equivalent to the force it takes to squeeze a tennis ball with one hand. Thinking about this gesture, think about repeating it at least 100,000 times in a day, that is the number of beats made by the heart in a day.
The heart of every human being begins to beat 4 weeks after his conception. From that moment on, he will finish his "work" only at the end of his life.
The heart can get sick from stress and strong emotions. The so-called heartbreak or broken heart, in fact, has a scientific explanation, which consists in the "increase of some hormones that paralyze the myocardium. The medical term for these pathological conditions is Takotsubo cardiomyopathy.
AND SISTOLIC RANGEEvery day the heart of an adult generates about 100,000 beats, pumping something like 7,500 liters of blood into the circulation; blood that is distributed through the 100,000km of blood vessels that feed organs and tissues.
In the blue whale the aorta (the largest artery of the organism) has a diameter of 23cm; through it the animal's heart pumps about 7,000 liters of blood per minute. When the blue whale is on the surface, its heart rate is 5-6 beats per minute, but as it sinks deeply, its heart slows down. beats.
or inaccuracies.
For instance…
- From the right ventricle there is a blood vessel that carries oxygen-poor blood, called the pulmonary artery, while blood vessels that carry oxygenated blood, called pulmonary veins, reach the left atrium. For many people, this may seem like an anomaly, as they associate arteries with vessels carrying oxygenated blood and veins with vessels carrying oxygen-poor blood.
In reality, however, all the vessels that branch off from the heart are arteries and all the vessels that reach the heart are veins, regardless of the type of blood contained. - About 5 cm from the heart, the aorta has a curved part, known as the aortic arch, from which three very important arteries originate: the anonymous, the left subclavian and the left common carotid.
- The coronaries, that is the vessels that nourish the myocardium, derive from two branches of the "ascending aorta. The ascending aorta is the first part of the aorta, before the aortic arch."
- In some people, the right atrium and left atrium communicate through an orifice, called the patent foramen ovale. This congenital heart defect is, in most cases, without consequences.
In the lungs, the same blood is loaded with oxygen and returns to the heart, through the pulmonary veins, in order to be distributed to the various organs and tissues of the body after being introduced into the aorta.
But if this occurs only at birth, how does the oxygenation of the blood and its distribution to the tissues take place before then?
As long as we are in the maternal womb, we do not have the possibility to breathe (and to oxygenate the blood), therefore it is our mother who supplies us with oxygenated blood.
That's how…
Maternal blood rich in oxygen reaches our body through the umbilical vein, which pours its contents into the inferior vena cava with which it is connected.
The inferior vena cava ends, as usual, in the right atrium, therefore the oxygenated blood will reach the heart through a different route from the "canonical" one mentioned above.
Once inside the right atrium, the oxygen-rich blood flows only minimally into the right ventricle, as it enters a small special opening, located between the right atrium and the left atrium and called the hole of Botallo.
With the direct passage from the "right atrium to" the left atrium, the oxygenated blood is ready to enter the aorta and, from there, to distribute itself in the various organs of the body.
At this point, an attentive reader may wonder what happens to the blood that reaches the right ventricle and the blood from the superior vena cava.
The answer is: they mix and enter the pulmonary artery, which, however, presents a deviation - called the ductus arteriosus - which puts it in direct communication with the aorta. As a result, the blood that reaches the right ventricle is also routed, in one way or another, into the main arterial system of our body.
Anatomically speaking ...
The aortic arch begins 5-6 centimeters after the ascending aorta (which is the very first part of the aorta), extends for a length approximately equal to the part that precedes it and ends where the descending aorta begins.
On its upper surface - generally in the central part of the curvature - it gives rise to three arterial branches of fundamental importance, which supply the upper limbs and the head with blood. These branches are called the left subclavian artery, the left common carotid artery, and the anonymous artery.
From the point of view of the relationships it establishes with nearby anatomical structures, on the anterolateral side it is related to various nervous structures (for example the left vagus nerve, the nerves of the anterior cardiac plexus, etc.); on the posterolateral side it is in contact with the trachea, the posterior cardiac plexus, the esophagus, the inferior laryngeal nerve, the thoracic duct and some lymph nodes; finally, on the lower face it comes into contact, for a while, with the pulmonary artery and , for another tract, with the left pulmonary artery.
, therefore they are considered true congenital pathologies, that is present from birth.
Specifying that anomalies of the aortic arch also refer to defects that can affect the three branches of the arch itself, the most well-known and studied variants of the aortic arch are:
- The double aortic arch
- The right aortic arch with a mirror image branching
- The right aortic arch with an anomalous branching
- The left aortic arch with an anomalous branching
- The cervical aortic arch
Since these are congenital defects (therefore inherent in the DNA), the researchers tried to identify what could be the genetic explanation of these diseases and found that, out of 100 people with an aortic arch defect, 20 have a genetic mutation on chromosome 22.
From an epidemiological point of view, defects of the "arch of the aorta" are quite rare pathologies. Furthermore, according to some estimates, they would represent about 1% of the possible congenital heart anomalies affecting the human being.


.jpg)