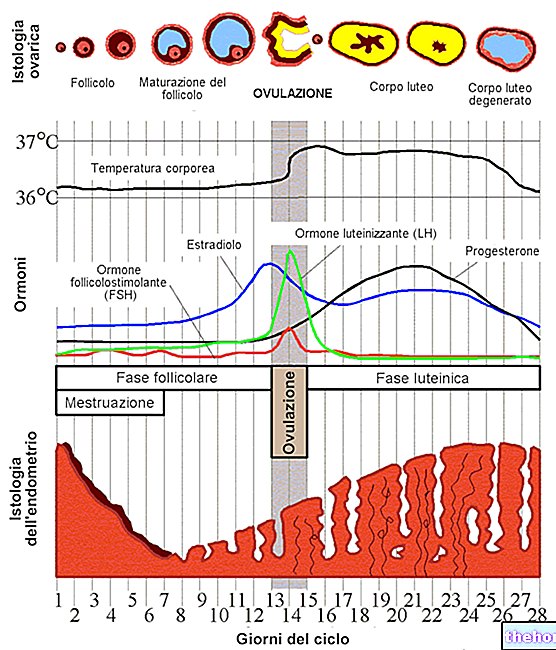
Bile is a digestive fluid produced by the liver and concentrated in the gallbladder, which pours it after meals into the initial tract of the small intestine, called the duodenum.

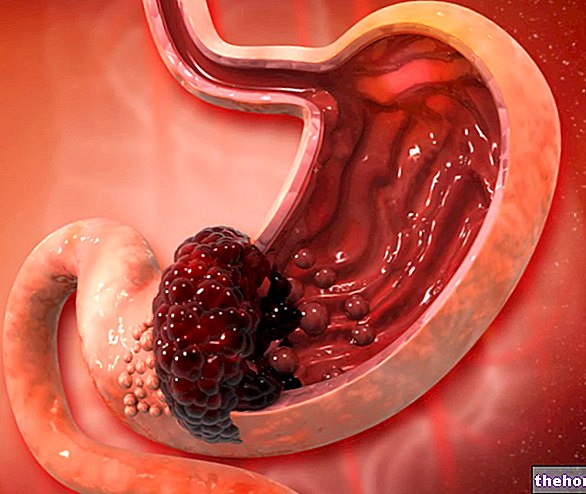
Figure: Biliary reflux: note the rise of the bile (green), from the duodenum where it is poured through the choledochus, to the stomach and from there to the esophagus. From the site: barrettsinfo.com
Bile reflux is caused by malfunctioning of the valves located between the stomach and duodenum and between the esophagus and stomach.
The excessive presence of bile irritates and inflames the gastric and esophageal mucous membranes. The main symptoms that follow are pain in the upper abdomen, heartburn and vomiting containing a yellow-green substance.
For a correct diagnosis, several tests are required, including gastroscopy.
The treatment is usually of a pharmacological type, while the use of surgery occurs only in special cases.
To better understand
The duodenum is the first part of the small intestine (or small intestine).
Separated from the stomach by means of a regulating valve called the pylorus, the duodenum represents a fundamental collection point for enzymes and digestive fluids (such as bile and pancreatic juice) that must intervene on the ingested food.
The esophagus is the cylindrical organ of the digestive system that directs food to the stomach. About 25-30 centimeters long and 20-30 millimeters wide, the esophagus begins at the level of the pharynx and ends at the level of the cardia (valve which regulates the passage of food in the stomach, also called cardial sphincter, gastroesophageal sphincter, lower esophageal sphincter (LES) or cardial valve).
WHAT IS BILE?
Bile is a yellow-green aqueous solution, produced by the liver and stored in the gallbladder (or gallbladder).
Composed of water (95%), electrolytes, lipids (bile acids, cholesterol and phospholipids), proteins and pigments (bilirubin), bile has various functions:
- Allows digestion and absorption of fats and fat-soluble vitamins taken from the diet (main function)
- Neutralizes the acidity of gastric secretions
- It stimulates intestinal peristalsis
- Eliminates the products resulting from the breakdown of red blood cells
- Eliminates toxic, pharmacological or endogenous substances (thyroid hormones, estrogens, etc.) present in the body
After a fat-containing meal, the bile leaves the gallbladder and enters the cystic duct first and then the choledochus. The latter is connected to the duodenum and allows bile to flow from inside.
BILIARY REFLUX AND ACID REFLUX (OR GASTROESOPHAGE REFLUX) ARE THE SAME WHAT?
Gastroesophageal reflux is the ascent of gastric juices (ie produced by the stomach) towards the esophagus. Gastric juices have an acid pH and this explains why we also speak of acid reflux.
Bile reflux and gastroesophageal reflux are two different pathological conditions, although the symptoms caused are very similar and often indistinguishable. It is also not uncommon for both types of reflux to occur in the same individual.
BILIARY REFLUX IN THE "ESOPHAGUS
As in the previous case, it is a valve defect that causes the bile to rise up in the esophagus.
In fact, when the cardia (in addition to the aforementioned pylorus) also loses its continence, the bile that goes back to the gastric level can also reach the esophagus.
Generally, this phenomenon is accompanied by a reflux of acidic juices, produced by the stomach; therefore there is the simultaneous presence of biliary and gastroesophageal reflux.
WHAT CAN DETERIORATE THE VALVES AND THEIR CONTAINING MECHANISM?
Malfunction of the pylorus and cardia valves may be due to:
- Complications after stomach surgery. Surgery for partial or total removal of the stomach (partial or total gastrectomy) and gastric bypass can lead to deterioration of the pylorus. As a result of this deterioration, the bile has a greater ease of ascending to the remaining upper compartment.
- Peptic ulcers. The presence of a peptic ulcer at the duodenal or gastric level can alter the functioning of the pylorus and cause the bile to rise towards the stomach and, possibly, also towards the esophagus.
- Cholecystectomy. Many individuals who have their gallbladder surgically removed are prone to bile reflux. The precise physiological mechanism of this is still unclear.
- Deterioration of the cardia or excessive stagnation of food in the stomach. They are the two main reasons why food, contained in the stomach, goes up the esophagus.
N.B: obviously, biliary reflux occurs in the esophagus when the pylorus is also damaged and allows the bile to rise back into the stomach.
WHEN TO SEE THE DOCTOR?
If you frequently experience the above symptoms and signs, it is advisable to contact your doctor and undergo an in-depth examination.
COMPLICATIONS
The bile contains substances which, if they often come into contact with the stomach and the esophagus, can deeply deteriorate the lining mucosa.
In particular, when acid reflux (equally persistent) is added to persistent bile reflux, the following complications can arise:
- Reflux esophagitis. It is inflammation of the esophagus due to continuous bile / acid reflux.
- Barrett's esophagus. It is the pathological condition in which the normal lining tissue of the esophagus is replaced by a tissue similar to that which lines the duodenum. This histological change makes the onset of an esophageal tumor more likely.
- Cancer of the esophagus. Researchers are still trying to scientifically prove the connection between bile / acid reflux and esophageal cancer. From the experiments carried out on animals, the link was evident; as regards man, however, there are still some outstanding points.
Again, a probe is used to insert into the esophagus.
Therefore, the upwelling of bile from the duodenum is a more difficult problem to manage than gastroesophageal reflux.
Therapy is usually of a pharmacological type; if, however, the drugs prove ineffective or there is a real risk of esophageal cancer, the doctor may resort to surgery.It is good to remember that potential surgical interventions are somewhat delicate and could involve several complications. Not by chance, before their execution, the patient is made aware of all the possible dangers that lie behind the operation.
PHARMACOLOGICAL TREATMENT
Medicines used in case of bile reflux are:
- Resins sequestering bile acids, such as cholestyramine. These drugs bind the bile acids poured from the gallbladder into the duodenum, in such a way as to prevent their reabsorption and favor their fecal excretion. Therefore, they reduce the acid content of the bile which causes irritation and inflammation.
- Prokinetics, such as domperidone and metoclopramide. They are used to promote the progression of food in the gastrointestinal tract.
Proton pump inhibitors and H2 receptor antagonists (antiH2), while representing the drug treatment of choice for acid reflux, have no appreciable effects in the case of duodenal-gastric biliary reflux.
SURGERY
The surgical operations that allow to reduce or stop bile reflux are:
- Roux-en-Y reconstruction (or esophagus-jejunal reconstruction on Y-loop according to Roux). Reserved for those who have undergone total gastrectomy, the operation basically consists in creating a drainage path for the bile.
- Laparoscopic fundoplication. It consists in wrapping and suturing the upper part of the stomach around the last section of the esophagus, in such a way as to oppose greater resistance to the reflux coming from the stomach.
SOME ADVICES
Although to a lesser extent than in situations of gastroesophageal reflux, do not smoke, eat moderate meals, do not lie down after eating, avoid foods that are too fatty or that promote gastric acidity (spicy foods, orange juice, tomatoes, caffeine-based drinks, chocolate etc), avoiding alcoholic beverages, losing excess weight, and sleeping with your head elevated are all good remedies for relieving bile reflux-induced symptoms.













.jpg)