Edited by Dr. Giovanni Chetta
INDEX
Premise
Scoliosis this unknown
Diagnosis of scoliosis
- Limits of Cobb's angle, radiographs and scoliosometer
Treatment of scoliosis
- Mild scoliosis
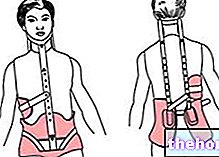
- Severe scoliosis
From biochemistry to biomechanics
- Extra-cellular matrix (MEC)
Connective tissue
- Connective tissue band
- Fascial mechanoreceptors
- Myofibroblasts
- Deep fascia biomechanics
- Viscoelasticity of the fascia
The specific motion of man
- Praise to the propeller
- Breech support
- Occlusal support (stomatognathic apparatus)
Myths about (idiopathic) scoliosis to dispel
Clinical case
- Introduction
- Materials and methods
- Results
- Discussion of the results
Conclusions
Bibliography
Premise
The aim of this work is to try to make a contribution of clarity, albeit necessarily partial, to the problem of idiopathic scoliosis and spinal and postural alterations in general, based on recent biomechanical and biochemical acquisitions.
After introducing the "canonical" concepts, commonly accepted, concerning scoliosis, I will move on to describe biochemical concepts that are the basis of biomechanical concepts that are now to be considered acquired. In turn, the description of the latter represents the foundations of the integrated treatment method, which I have in team with other professionals, used for the real clinical case given as an example.
Scoliosis this unknown
Scoliosis - from the Greek skolios which means crooked, twisted - represents a deformation of the spinal column that has always caught the attention, especially for its strong aesthetic impact. This alteration (previously considered two-dimensional) is usually three-dimensional and constant, and is highlighted in particular way on the frontal plane; characteristic signs of scoliosis are in fact the lateral convexities / concavities of the rachis.
Scoliosis affects about 3% of the population with female prevalence (5: 1) and in the childhood-adolescent period (over 80%). In most cases it occurs at the beginning of pubertal development and tends to evolve up to bone maturation.In important scoliosis, however, evolution can persist even if very slowly.
Normally scoliosis does not cause pain except in the adult if an important degree of spinal deformation is reached which can lead, in some cases, to significant organic dysfunctions such as cardio-respiratory ones. Scoliosis is severe in less than 0, 5 per thousand of cases (source: www.isico.it).

The same differentiation between structural scoliosis (dysmorphism) and scoliotic attitude (paramorphism) it can often represent a diagnosis, therefore a poorly specific prognosis, and consequently entailing ineffective re-educational treatments. Structural scoliosis is defined as such if we are in the presence of a structural alteration of the vertebrae, that is, there is the detection of some deformed vertebrae. The abnormal curvatures of this scoliosis are therefore more persistent and more resistant to correction.
In reality, it must be considered that bone tissue, being part of the large family of connective tissues, has a specific peculiarity: viscoelasticity. In fact, bone tissue can be considered as a composite material consisting largely of rigid hydroxyapatite (HAP) particles inserted in a flexible (elastic) matrix made of collagen fibers. The anisotropic form of these mineral particles is one of the probable causes of the anisotropic mechanical properties (the "anisotropy represents the characteristic of a solid for which the physical properties assume different values depending on the direction in which they are measured) of the cortical bone tissue. L" evident viscoelastic behavior shown by the bone tissue is related to the viscoelasticity of the collagen fiber of the bone matrix (Clienti et al, 2007). Like all connective tissues, therefore, bone is also malleable. As demonstrated by J. Wolff as early as 1892 with his law, bone deformation occurs in the directions and on the basis of the mechanical stimuli (thrusts and / or tractions) that it undergoes in a preponderant way (both under the quantitative and temporal aspect). The mechanical load therefore represents the variable that conditions the architecture of the bone. Specifically, the lack of collagen fibers determines a greater fragility of the bone while the lack of calcium increases the flexibility of the bone. Therefore the malleability of the bone it is, as a rule, maximum in the growth phase and in the osteoporotic phase.
The probability that a scoliotic attitude (paramorphism) evolves over time into dysmorphism (structural scoliosis) is therefore to be considered high.
Wolff's law
The trabeculae are arranged according to the main directions of the stresses and their thickness and the spaces between them vary as the intensity of the load varies. Any change in function or shape in the bone is accompanied by variations in its internal architecture, as well as by alterations secondary to the external conformation, both linked to precise formulations
It is believed that the scoliotic process predominantly (70% of cases) starts with one or two primary curves (also called main or primitive) which can be followed by other minor compensation (Stagnara, 1985), such as to allow the subject to pursue the primary need to look towards the horizon while walking.
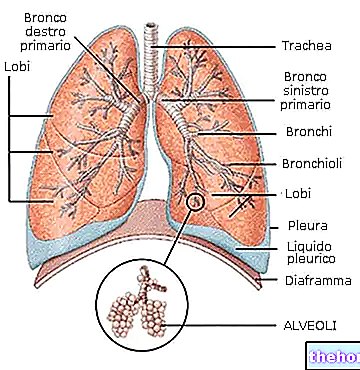
The scoliotic alteration, like all spinal deformations, involves, in addition to the vertebrae and the relative joints, the intervertebral discs, the ligaments, the myofascial system and the internal organs. All this is therefore capable of causing structural and functional problems , as well as aesthetic, which can evolve negatively over time unless appropriate action is taken.
Other articles on "Scoliosis - Causes and Consequences"
- Scoliosis Diagnosis
- Prognosis of scoliosis
- Treatment of scoliosis
- Extra-Cellular Matrix - Structure and Functions
- Connective tissue and Connective fascia
- Connective Band - Features and Functions
- Posture and tensegrity
- Man's motion and the importance of breech support
- Importance of correct breech and occlusal supports
- Idiopathic Scoliosis - Myths to Dispel
- Clinical case of Scoliosis and Therapeutic Protocol
- Treatment Results Clinical Case Scoliosis
- Scoliosis as a natural attitude - Bibliography