Like the one that feasts on plaque, tartar and gum pockets, the lingual microflora produces volatile sulfur compounds (especially hydrogen sulfide and methyl mercaptan) and other substances responsible for bad odor, such as some short-chain fatty acids.
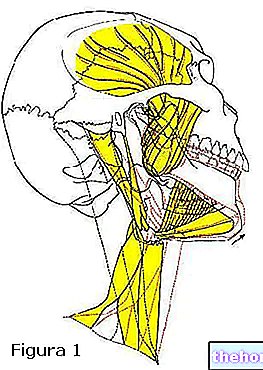
For this reason, simple tooth brushing is not enough to combat bad breath; attention must also be paid to sites that are difficult to clean with common oral hygiene practices, such as the surface of the tongue.
Cleaning the tongue is not only a formidable ally in the fight against halitosis; the lingual patina is in fact a reserve of microorganisms capable of influencing the bacterial flora of the entire oral cavity. A clean tongue therefore means a slowdown in the formation of bacterial plaque and its accumulation, which consequently reduces the risk of tooth decay and gingivitis.
Cleaning the tongue (brushing) can be done using the classic toothbrush or - preferably - using a special tool called lingual scraper. The cleaning technique with the toothbrush involves positioning the instrument horizontally, keeping the handle perpendicular to the center line of the tongue, which must be extruded (ie made to come out of the mouth, so as to be able to reach the posterior areas of the lingual dorsum, where there is the greatest number of bacteria). The toothbrush should be pushed down with a slight pressure towards the tip of the tongue. on the sides and at the base of the tongue; it is also possible to use the rubber back part of the brushes specially designed to facilitate lingual cleaning.
The scraper, on the other hand, must be passed back and forth on the surface of the tongue with a light but firm movement, always proceeding from the inside to the tip of the tongue.
in the treatment of halitosis is rather debated, above all due to possible methodological errors in published studies and conflicts of interest deriving from research funding by manufacturers.
If the toothbrush acts mechanically through the action of rubbing the bristles, the mouthwash intervenes above all chemically. The mechanical washing action of the rinses, in fact, could also be obtained using simple tap water, so that the alleged additive advantages of mouthwashes would derive by their particular chemical composition.
The active ingredients contained in mouthwashes can be of different types; some, such as chlorhexidine, have a certain antiseptic action, useful for directly decreasing the bacterial load of the microbial flora. Other products - like most of the commercial mouthwashes available at the supermarket - only exert an "odor masking action", thanks to the content of aromatic substances such as menthol; the effectiveness of these products is clearly short-lived and even - although essential oils are attributed a certain antibacterial activity - alcohol-based ones could worsen halitosis due to their dehydrating effect.
Other substances contained in mouthwashes - such as zinc salts - are able to neutralize the volatile sulfur compounds responsible for bad odor.
Antiseptic agents, such as triclosan, cetylpyridinium chloride, and chlorhexidine, are slightly more effective, but have side effects; chlorhexidine, in particular, tends to stain the teeth and for this reason spray products against halitosis are available to be applied directly on the surface of the tongue, thus reducing the contact of chlorhexidine with the teeth.
To learn more: Mouthwash for Inflamed Gums: 5 Best according to Amazon Reviews.These results have been confirmed by other studies, so today it is believed that only 5-8% of cases of halitosis can be attributed to non-oral causes.
Therefore, the widespread opinion that bad breath mainly depends on gastrointestinal disorders is absolutely unfounded. Almost always the problem depends "only" on poor oral hygiene. For example, tooth brushing alone is not enough; especially in the presence of halitosis it is also important to take care of the brushing of the tongue, in order to break down the microorganisms responsible for the production of the volatile sulfur compounds at the base of halitosis.
As well as mechanically, the tongue and teeth can also be "cleaned" chemically; in particular, rinses and gargles based on antiseptic chemicals, such as chlorhexidine, or capable of masking bad odors, such as menthol, can help improve the situation. However, it should be emphasized that the effective anti-halitosis action of mouthwashes is debated.
The correct use of the toothbrush must then be combined with the use of dental floss to also clean the spaces between tooth and tooth, where the bristles of the toothbrush do not reach. Periodic visits to the dentist allow you to remove any deposits of tartar, preventing gingivitis and periodontitis; the dentist it can also assess whether the patient's oral hygiene is actually adequate or whether it needs to be improved.
To learn more: Children's Toothpaste: the 5 Best according to Amazon Reviews that provide sulfur, such as garlic, onion, leeks, broccoli and spices such as curry. In fact, whether it comes from the sulfur absorbed in the intestine and eliminated with the breath, or whether it comes from the oral cavity, the bad smell is largely determined by volatile sulfur compounds (the bacteria in the mouth produce these substances by metabolizing amino acids containing sulfur present in the saliva and food residues). It should also be remembered that bingeing on very sulfur-rich foods can cause bad breath problems for up to 72 hours after a meal.
Food aside, bad breath on waking generally depends on the physiological decrease in salivary flow at night. During sleep, the low secretion of saliva is in fact important to avoid frequent swallowing movements. Unfortunately, this dry mouth impoverishes the mouth of an important protection against halitosis, represented precisely by saliva; this, in fact, cleanses the teeth by removing food debris, bacterial residues and epithelial cells, as well as buffering acidity.
For what has been said, in the morning, especially at the lingual level, there is an "important presence of microorganisms that produce substances responsible for halitosis.
In addition to facilitating bacterial proliferation and bad breath, the reduction in nocturnal salivary flow facilitates the onset of carious processes, so proper oral hygiene before sleeping is very important.
The same sulfur contributes to characterize the smell of cabbage and spoiled eggs.
The icing on the cake, sulfur is also responsible for bad-smelling flatulence eliminated after taking such foods.
, some systemic diseases (eg Sjogren's syndrome), certain radiotherapy interventions and the intake of particular drugs, can cause a marked reduction in salivation, generating problems of oral dryness and an increased incidence of dental pathologies.
There are a number of local agents available for the treatment of dry mouth (called xerostomia). Among these, some stimulate the function of the residual salivary glands (sialagogues), while others act as real saliva substitutes. For example, a simple chewing-gum is able to significantly increase the production of saliva, also exerting an "antibacterial and pH rebalancing action if it contains substances such as xylitol and chlorhexidine. There are also systemic drugs, such as pilocarpine. capable of stimulating the production of saliva. However, when the number of functioning salivary glands is greatly reduced, all these stimulant products are ineffective. In this case the use of saliva substitutes becomes particularly suitable.
Modern saliva substitutes are water-based products containing substances - such as hydroxymethylcellulose, carboxymethylcellulose and electrolytes - capable of reproducing the consistency and lubricating action of saliva; the latter, however, also contains antibacterial substances, such as lysozyme, so when possible the use of sialagogues is generally preferred.
Saliva substitutes generally come in the form of nebulizers or rinse solutions. They are considered palliatives of limited efficacy and require several daily administrations (at least three or four). As an alternative to these products, the habit of frequently sipping water, both during meals and during the rest of the day, certainly has a beneficial effect. Compared to water, it was seen as the relief given by the humectant action of saliva substitutes. have a duration of approximately double.
), eaten with the peel.This type of apple is characterized by a lower sugar content than other varieties; moreover, if eaten while still unripe, its sugar content is lower than that of ripe fruit.
The consumption of the apple with the peel is also very important; in fact, just like the bristles of the toothbrush and dental floss, during chewing the peel of the apple contributes to the mechanical cleaning of the dental and periodontal apparatus.
Another characteristic of the green apple is the high concentration of malic acid, responsible for the sour taste of the fruit. Like all acid substances, malic acid helps whiten teeth; however, it can also damage the surface of the enamel and the underlying dentin, which can cause problems for those with sensitive and poorly mineralized teeth. apples are often referred to as foods with a moderate content of fluorine, a known mineral with a preventive effect against the fragility of the enamel and tooth decay.
A rinsing of the mouth with water after the consumption of an apple can however help to bring the oral pH back to normal, preventing damage to the enamel and completing the cleansing action of the fruit.
which blocks ovulation, creating many problems for pregnant women.
Progesterone also has a "pro-inflammatory action, so it predisposes to the onset of gingivitis, that is" inflammation of the gums, whose bleeding is the characteristic symptom of this condition.
Furthermore, the hormonal interactions of pregnancy favor an increase in periodontal pathogenic species, weaken the immune defenses, acidify saliva and increase vascularization in the gums. For this reason, during gestation it is not uncommon to notice variations in the color of the gums from pale pink to dark pink; gums which in pregnant women also tend to be more swollen and prone to bleeding. To worsen the situation there is also the tendency to eat small and frequent meals, often sweet, either to counteract the sense of nausea, or for the typical "cravings" of pregnancy.
It is no coincidence that there is a saying that each child would cost a mother a tooth.
Beyond the idioms and this natural predisposition to gingivitis, it should be noted that healthy gums are unlikely to bleed during pregnancy. When pregnant women notice bleeding while brushing or flossing, it most likely means that the gums were somehow predisposed prior to pregnancy; essentially there was already some underlying inflammation that was amplified by hormonal changes.
In case of gum bleeding during pregnancy it is therefore important to have a dental visit, for professional hygiene and to receive advice on proper oral hygiene at home. This recommendation becomes even more important considering that in the literature there are many studies that show a significant correlation between gingival - periodontal diseases, and gestational complications such as premature birth For example, we have seen how a pregnant woman with periodontitis is 7.5 more likely than the average to give birth to a premature and underweight baby.
a worm born in the mud would have begged Poseidon to allow him to live between the teeth and gums of man, where residues of food and drink abound. Obtained divine permission, the worm settled in the human mouth, starting to dig tunnels and caves.As early as 400 BC Hippocrates urged not to believe the story of the worm and recommended to clean the teeth and gums every day to avoid cavities and toothache. But how to treat oral hygiene with the scarce means available in those times? Coal, alum, animal bones, shells of molluscs, bark and various types of plant extracts were the most used ingredients to prepare pastes and mouthwashes for rinses.
In "ancient Mesopotamia, for example, people brushed their teeth with a mixture of bark, mint and alum. In ancient India, instead, they used a mixture based on extracts of barberry and pepper. In Egypt, during the twelfth dynasty, the princesses used verdigris, incense and a paste based on sweet beer and flowers such as crocus. All cultures of antiquity knew toothpicks, made of wood, rachis or other materials.
Hippocrates himself, for cleaning his teeth, recommended a mixture of salt, alum and vinegar as a mouthwash.
In the literature of Pliny the Elder (23 - 79 AD) the uses of various plants for the well-being of the oral cavity are reported; mastic leaves, for example, rubbed against aching teeth, and their decoction was considered useful for inflamed gums and sagging teeth. The dried resin of the mastic grown on the island of Chios was and still is considered an excellent refreshing chewingum, which perfumes the breath giving a sensation of freshness and cleanliness. The thorns of the plant were used as toothpicks and in their absence the use of goose feathers or different birds was recommended.
In Arab countries, the siwak, a root or wood stick obtained from the arak plant, was and still is widespread as a toothpick (Salvadora persica); the Maya of Central America, on the other hand, chewed the "Chicle", given by the latex of the Sapotilla tree (Manilkara zapota), which has long been an ingredient in modern chewingum.
Pliny himself indicated olive oil as an effective mouthwash against tooth infections.
Pliny was also among the first to report the use, to effectively rinse teeth and gums, of a natural and extremely biological mouthwash: urine. Thus, in addition to cleaning clothes, the use of urine aged a few days to whiten teeth was quite widespread among the ancient Romans.
Among the peoples of Muslim origin, the care of oral hygiene also assumed a religious significance, given that from 600 AD the word of Muhammad imprinted in the Koran recommended: "Keep your mouth clean because praise to God passes from there!" his part, The Holy Roman Church, promised: "Whoever prays to the holy martyr and virgin Apollonia, on that day will not be affected by toothache." It was thus that, in the thirteenth and fourteenth centuries, Apollonia became the patron saint of those who suffered from toothache.
In the history of oral hygiene, an important role is played by mouthwashes. The ancient Egyptian, Chinese, Greek and Roman cultures were already steeped in recipes and folk remedies for dental care and for freshening the breath. Ingredients included materials such as charcoal, vinegar, fruit and dried flowers; it seems that the Egyptians used a highly abrasive mixture of pulverized pumice and wine vinegar. The Romans, as mentioned, preferred urine, mainly used as a mouthwash due to the presence of ammonia.
The first evidence of a real toothbrush with bristles, similar to today's one, dates back to 1500 in China.The fibers, however, being natural (pig hair attached to a bone or a bamboo stick), were too soft and easily deteriorated, becoming a receptacle for bacteria. Meanwhile in Europe, in the middle of the Middle Ages, the fashion of not washing was raging, supported by medical and religious influences; the Sun King, who took no more than two baths in his entire life, was already completely toothless at a young age. At that time, fans, so much appreciated by noblewomen, were the ideal remedy to spare the interlocutor the sight of smiles disfigured by caries and the pestilential smell of his own breath. civet, animal musk and amber, the toothache was tried to be remedied with equally unique recipes, passed off as miraculous remedies by the merchants of the time. "A porridge of wolf and dog dung, mixed with rotten apples, helps in case of toothache" or: "Fallen teeth grow back if you massage your jaw with hare's brain" or "The best thing is to fight tooth worms with a mixture of roasted hare's head and finely chopped sheep's hair ».
With the advent of the first microscopes, the theory of the tooth worm was definitively shelved. Antony van Leeuwenhoek discovered the bacteria by observing under the microscope residues of plaque and tartar taken from his own teeth. After observing the bactericidal effects of alcohol, Leeuwenhoek tested the partial ineffectiveness of mouth rinses with brandy and vinegar, concluding that the mouthwash probably did not reach the microorganisms or did not stay in contact long enough to kill them.
An important step forward was made around the mid-1800s, when fluoride-based candies sweetened with honey were put on the market. In the same period began the production of toothbrushes and pastes containing fluoride and sodium salts similar to today's toothpastes. In 1872, Samuel B. Colgate invented the first modern toothpaste based on mineral salts and refreshing essences. In 1938 America produced the first "Dr. West's Miraculous Wisp Toothbrush" with synthetic fibers (nylon).
sold at the supermarket) have an effect mainly masking halitosis rather than curative; this is because they contain substances (mostly essential oils) that exert a masking effect on bad smells; in fact, the antibacterial activity of xylitol and the essential oils contained in mouthwashes is low, both due to the low concentrations, and above all due to the low contact time with teeth and oral mucosa. In the presence of bad breath, therefore, the mouthwash does not cure the cause of the problem, but simply cancels the effects. The real results in the fight against halitosis are obtained by eliminating the bacteria that produce these odors, and to do so nothing is more effective than the mechanical action of the toothbrush, dental floss and scrapers for cleaning the tongue. The chemical killing of these bacteria can be obtained with medicated mouthwashes (sold in pharmacies), based on antiseptic substances. However, these products have important side effects; the best known is linked to chlorhexidine, an antibacterial active ingredient present in recommended medicated mouthwashes. in the presence of chronic gingivitis, very aggressive carious pathologies and important problems of the periodontium; chlorhexidine, in fact, tends to dirty the teeth and tongue with yellow-brown spots that require "outpatient hygiene to be removed." Furthermore, inappropriate use of chlorhexidine creates bacterial resistance and inflammation of the mucous membranes. Other antiseptic agents, such as triclosan, have even been banned for use in mouthwashes in some countries due to potential side effects.
Returning to cosmetic mouthwashes, one of the greatest risks associated with their use derives from the presence of ethyl alcohol among the ingredients. Ethanol is added above all to enhance the flavor of the product rather than for the real antibacterial properties. However, the presence of alcohol can induce side effects, since ethanol tends to dry and irritate the oral mucosa, causing stomatitis from irritation and hypersensitivity. Furthermore, according to some studies, the alcohol contained in mouthwashes increases the risk of cancer of the mouth and oral cavity.
All these warnings should suggest the importance of submitting any oral disorders to a dentist, to identify the causes and possibly choose the most suitable mouthwash for your needs.
, better known as cetylpyridinium chloride (INCI Cetylpyridinium chloride). Due to its chemical and functional characteristics, CPC is a cationic disinfectant belonging to the group of quaternary ammonium salts.In the United States, cetylpyridine was used as an anti-plaque mouthwash as early as 1940. This active ingredient has in fact proved effective in the disinfection of the oral cavity and in the prevention of caries and gingivitis, thanks to its bactericidal activity against a wide spectrum of bacteria in the cavity. oral, especially gram-positive ones. For the same reason, cetylpyridine is also useful in case of bad breath problems of oral origin.
Cetylpyridinium chloride acts by binding to the bacterial wall and causing its lysis, thus causing cellular components to escape with metabolic alterations up to the death of the microbe. The ability to bind to bacterial cell membranes depends on the cationic (positively charged) surface of the CPC; therefore, in the formulation of products containing cetylpyridine it is necessary to respect this characteristic making it stable. Some anionic detergents, widely used in the formulation of toothpastes, such as Sodium-lauryl-sulfate (SLS), interact with CPC by inactivating its positive charge and consequently limiting its antiseptic activity. For this reason, some authors recommend waiting at least 30 minutes between brushing your teeth with toothpaste and using a cetylpyridine-based mouthwash.
Recently, the use of cetylpyridine is finding a certain space in medicated products for oral hygiene, in combination with chlorhexidine (CHX). This combination would make it possible to reduce the doses of chlorhexidine necessary to produce the desired antibacterial effect, thus also limiting the side effects of the latter in terms of dental discoloration.
Cetylpyridinium chloride is used in concentrations between 0.03% and 0.1%. At therapeutic concentrations it has no toxic effects. Among the undesirable effects, dental pigmentations and, in sporadic cases, local irritation with burning sensation in the oral cavity have been described. However, it seems that the risk of dental stains is considerably lower than with the use of chlorhexidine.
Cetylpyridine is also present in hand sanitizers, medicated products for intimate hygiene, deodorants and pharmaceutical products (eg sore throat tablets, or acne products).
. Chronic inflammation, in fact, releases a whole series of inflammatory cytokines in the bloodstream that favor the formation and / or rupture of atherosclerotic plaques, in turn responsible for fearful cardiovascular diseases such as heart attack, ischemic stroke and heart disease Not surprisingly, recent research has shown that if the health of the gums improves, it also slows down the formation of atherosclerotic plaques, and vice versa.
However, the relationship between poor oral hygiene and other diseases still needs to be clarified. For example, some studies have shown a correlation between chronic inflammation of the gums (chronic gingivitis) and Alzheimer's disease, while on the oncological front, periodontal disease could, perhaps, increase the risk for certain types of cancer, such as that of the colon or pancreas.