
Figure: representation of pulmonary fibrosis; note the presence of scar tissue (greenish) in the left lung. From the site: lungsandyou.com
There are two forms of pulmonary fibrosis: the idiopathic form, for which a precise trigger has not yet been found, and the secondary form, for which, instead, several determining factors have been identified.
Typical symptoms of pulmonary fibrosis are wheezing, dry cough, weight loss and a sense of fatigue.
Diagnosis requires a fairly long process, consisting of several examinations and tests.
Unfortunately, it is impossible to recover from pulmonary fibrosis. The only treatments currently available serve to relieve symptoms and improve the quality of life of the sick.
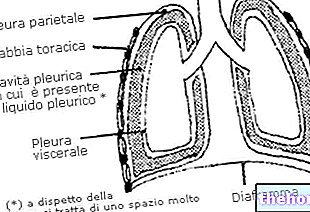
A lung affected by fibrosis is therefore a lung that is not very elastic, hard, and covered with retracting scars that "crush" the alveoli, preventing normal breathing.
What are the alveoli?
The alveoli are small cavities in the lungs, where gas exchanges between the blood and the atmosphere take place. Inside them, in fact, the blood is enriched with the oxygen contained in the breathed air and is "freed" of the carbon dioxide discarded by the tissues, after their spraying.
, in the second of secondary pulmonary fibrosis.IDIOPATHIC LUNG FIBROSIS
In medicine, a disease is called idiopathic when it arises for no identifiable reason.
Researchers have proposed various theories regarding the causes of idiopathic pulmonary fibrosis, but none of these, so far, have been proven with sufficient scientific evidence.
Most of the investigations involved:
- Cigarette smoke.
- Particular viral infections, caused by the Epstein-Barr virus or the hepatitis C virus.
- Coal powders and metal powders.
- Factors of a genetic / hereditary nature, linked to the transmission of the mutated gene for the so-called surfactant protein C (N.B: surfactant is a fundamental substance for the proper functioning of the lungs).
SECONDARY LUNG FIBROSIS
In medicine, a disease is compared to the secondary term when it appears after the occurrence of a particular condition, which can be pathological or non-pathological.
Secondary pulmonary fibrosis can arise due to:
- Prolonged exposure to toxic substances in the workplace. Harming lung health: asbestos fibers (which also cause tumors, such as pleural mesothelioma and lung cancer); the stone, marble and wood dust emitted by sandblasters; the excrement of some animals and some birds; the powders produced by stored grain and flours; finally, silicon powders.
- Cycles of anticancer radiotherapy. Radiation therapy performed for breast and lung cancers can have side effects, especially if it is very prolonged and the amount of ionizing radiation emitted is high. The consequences of radiotherapy can appear even months or years after anticancer treatment.
- Medicines used to treat cancer (chemotherapy), heart problems and bacterial infections (antibiotics). Among the chemotherapy drugs that are dangerous for the lungs, methotrexate, cyclophosphamide and busulfan are reported.
Medicines for heart problems include amiodarone (an antiarrhythmic) and propranolol (an antihypertensive and antiarrhythmic).
Finally, among the antibiotics, nitrofurantoin, bleomycin and sulfasalazine are potentially harmful. - Infectious or autoimmune diseases. Infectious diseases associated with pulmonary fibrosis are tuberculosis and pneumonia (both bacterial and viral). The offending autoimmune diseases, on the other hand, are systemic lupus erythematosus, rheumatoid arthritis, sarcoidosis, Wegener's granulomatosis and scleroderma.
RISK FACTORS
According to some statistical surveys, pulmonary fibrosis is more frequent among: the elderly; heavy smokers; those who work in farms, mines, carpentry or metallurgical factories; those who have undergone radiation therapy for lung or breast cancer; those who have used chemotherapy drugs; and, finally, individuals with a family history of pulmonary fibrosis.
EPIDEMIOLOGY
Pulmonary fibrosis is a widespread disease all over the world: it can affect men and women of any ethnicity.
Its idiopathic form seems to have an "annual incidence of 6-16 cases per 100,000 people. Its secondary form, on the other hand, has an extremely variable" incidence from country to country, as it depends on how much people are exposed to the triggering causes .
For both forms, the most affected individuals are those between the ages of 50 and 70, although it must be said that the disease can arise at any age.
Pulmonary fibrosis makes no distinction between males and females; in fact, it afflicts both sexes with a very similar frequency.
The signs and symptoms typically associated with pulmonary fibrosis are:
- Dyspnea, or difficulty in breathing
- Dry cough
- The feelings of fatigue and weakness
- Weight loss for no reason
- Chest pain
- Muscle and joint pains
The severity of these manifestations varies from person to person: in some subjects, the symptoms are very marked immediately, in others it is initially moderate and gradually worsens over several months / years.
The evolution of pulmonary fibrosis would seem to depend on the triggering causes.
COMPLICATIONS
A prolonged situation of pulmonary fibrosis can lead to the onset of serious complications, such as pulmonary hypertension, cor pulmonale, respiratory failure and lung cancer.
Learn more about complications
Pulmonary hypertension is the increase in pressure inside the arterial vessels that carry the blood to be oxygenated to the lungs. In the presence of pulmonary fibrosis, this pressure increase depends on the compression that the scar tissue exerts on the alveoli and alveolar capillaries, in which carbon dioxide-oxygen exchange takes place between blood and atmosphere; this compression causes an obstruction and an obstacle to the free flow of blood. Pulmonary hypertension is a serious problem that tends to get worse over time and can lead to death.
Pulmonary heart is a very serious heart disease, triggered by pulmonary hypertension and characterized by an enlargement of the right ventricle of the heart (NB: the right ventricle is the contractile cavity of the heart that pumps blood into the arteries directed to the lungs, ie the arteries Its appearance causes worsening of dyspnoea.
Respiratory insufficiency is usually the final consequence of severe pulmonary fibrosis. It causes severe shortness of breath and poor oxygenation of the circulating blood (severe hypoxemia). The lungs, in these situations, become extremely rigid and become covered with numerous retracting scars.
Finally, lung cancer is one of the most common neoplasms that can arise among pulmonary fibrosis patients.
OBJECTIVE EXAMINATION
During the physical examination, the doctor visits the patient, gathering from the latter information on the complaints and auscultation of the chest with a phonendoscope.
IMAGE DIAGNOSTICS
The most suitable diagnostic imaging tests in the case of pulmonary fibrosis are chest X-rays, CT scans and echocardiography.

Figure: Comparison of X-ray images of healthy (left) and fibrosis-affected (right) lungs
The chest X-ray (or chest X-ray) and the CT scan (or Computerized Axial Tomography) both allow to visualize the main anatomical structures of the chest: therefore the heart, lungs, main blood vessels, most of the ribs and a portion of the vertebral column . The second, however, is more precise than the first, because it shows more clearly the extent of the scar tissue present in the lung.
The echocardiogram is used to evaluate the state of health of the heart and if the latter is affected by some anatomical anomaly (for example the cor pulmonale).
Attention: chest x-ray and CT scan expose the patient to a certain dose of ionizing radiation (X-rays) which are harmful to health.
TEST FOR THE EVALUATION OF THE FUNCTIONALITY OF THE LUNGS
The tests to evaluate how the lungs work are: spirometry, oximetry and the stress test.
Spirometry. Fast, practical and painless, spirometry records the inspiratory and expiratory capacity of the lungs, and the patency (ie the opening) of the airways passing through the latter.
Oximetry. As simple and straightforward as spirometry, it measures oxygen saturation in the blood. It is carried out with an instrument, called an oximeter, which is applied to a finger or to an earlobe (in both cases, these are highly vascularized areas, therefore particularly suitable for the purpose).
Stress test. It consists in evaluating how the heart rhythm, blood pressure and breathing of the patient vary while the patient is performing a more or less intense physical activity.
LUNG BIOPSY
Lung biopsy consists in taking and analyzing in the laboratory a small sample of lung tissue, coming from the patient. The sampling can be done by:
- Bronchoscopy. During bronchoscopy, doctors collect lung tissue with an instrument, the bronchoscope, introduced through the nose or mouth. The bronchoscope is basically a very thin, rather flexible tube equipped with a fiber optic camera for orientation inside the lung cavities.
The passage of the bronchoscope can irritate the airways crossed; furthermore, the quantities of tissue removed may not be sufficient for the diagnosis. - Bronchoalveolar lavage. During bronchoalveolar lavage, the doctor always uses a bronchoscope, but, unlike the previous procedure, injects a saline solution into the lungs which is promptly sucked in after a few moments. This operation allows a larger sample of cells to be taken than bronchoscopy alone, although not always sufficient.
- Surgical intervention. Surgery to collect a lung sample requires general anesthesia and involves making two or three incisions on the side. Through these micro-openings, the surgeon introduces a camera (connected to an external monitor and essential for l "orientation) and the tools necessary for sampling.
A surgery of this kind is very bloody and dangerous, however it is the procedure that, from a diagnostic point of view, guarantees the most useful information.
Because scar tissue is permanent and its formation almost unstoppable, scar fibrosis is an incurable and irreversible disease. However, thanks to some drugs, oxygen therapy and respiratory rehabilitation, it is possible to alleviate the symptoms and slow down their progression, thus also improving the patient's quality of life.
The hypothesis of a lung transplant, which is a very delicate surgery with an uncertain outcome, is taken into consideration only in extreme cases and when the aforementioned treatments have proved completely ineffective.
PHARMACOLOGICAL THERAPY
Many patients with pulmonary fibrosis (both idiopathic and secondary) are treated with corticosteroids and immunosuppressants, because these are the only drugs tested to have any effect on symptoms and disease progression.
Corticosteroids are powerful anti-inflammatories which, when taken for long periods of time and in high doses, can lead to serious side effects (osteoporosis, diabetes, cataracts, hypertension, obesity, etc.).
Immunosuppressants, on the other hand, are medicines particularly indicated in the presence of an autoimmune disease, as they lower the body's immune defenses.
Drugs indicated in case of pulmonary fibrosis
Corticosteroids
Immunosuppressants
Prednisone
Methotrexate
Cyclophosphamide
Azathioprine
Penicillamine
Cyclosporine
OXYGEN THERAPY
Oxygen therapy is the administration of oxygen through special medical instruments (some of which are also portable). This intervention is necessary when there is a need to increase the amount of oxygen circulating in the blood.
In case of pulmonary fibrosis, oxygen therapy offers various benefits, as:
- Makes breathing easier
- Reduces the possibility of hypoxemia (low oxygen levels in the blood)
- It reduces the blood pressure within the right compartment of the heart (preventing complications such as pulmonary hypertension and cor pulmonale).
- It improves the night's sleep, therefore also the quality of life.
Attention: oxygen therapy improves symptoms, but unfortunately does not slow down the formation of scar tissue inside the lung.
RESPIRATORY REHABILITATION
Respiratory rehabilitation consists in having the patient practice a series of motor exercises (exercise bike, climbing stairs, walking, etc.), in order to improve tolerance to efforts and reduce the severity of dyspnea.
This treatment, like oxygen therapy, also mitigates the symptoms but does not stop the progression of the disease.
LUNG TRANSPLANT
Lung transplantation is the procedure of replacing the diseased lung with another healthy one from a compatible donor. Given the considerable invasiveness and the more than fair probability of failure of the operation (organ rejection), lung transplantation is an operation practiced only in extreme cases and when all the other solutions mentioned above have not provided any benefit.
SOME TIPS ON THE LIFESTYLE
For patients with pulmonary fibrosis, doctors recommend:
- Quitting smoking: although a certain connection between cigarette smoking and pulmonary fibrosis has not yet been scientifically demonstrated, tobacco reduces the functionality of the lungs and is the cause of many other lung diseases (such as lung cancer).
- Avoid secondhand smoke: because it is as harmful as active smoking.
- Contact a dietician to plan a balanced diet. Patients with pulmonary fibrosis, in fact, are subject to a decrease in body weight, as, due to respiratory problems, they have difficulty in feeding properly.
- Get vaccinated against influenza (influenza vaccine) and pneumonia (pneumococcal vaccine), as these are two respiratory infections that could further worsen the symptoms.

.jpg)

















-nelle-carni-di-maiale.jpg)




