Definition and classification
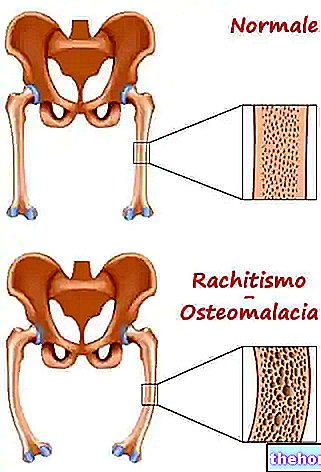
Rickets is a skeletal disease (osteopathy) with childhood onset, caused by a defect in the mineralization of the bone matrix and potentially responsible, in an advanced stage, for bone deformities and fractures. On the basis of the etiopathogenesis of rickets it is possible to classify it in:
- Rickets due to altered intake of vitamin D (calciferol):
- deficient rickets
- rickets from chronic intestinal malabsorption
- Rickets due to impaired hepatic metabolism of vitamin D:
- rickets in hepato-biliary diseases (hepatic osteodystrophy)
- rickets from chronic treatment with anticonvulsant drugs (barbiturates)
- Rickets due to impaired renal metabolism of vitamin D:
- familial hypophosphatemic rickets
- Vitamin D-dependent rickets type 1
- renal osteodystrophy
- rickets from tubulopathies
- oncogenetic rickets
- Vitamin D reduced action rickets:
- Vitamin D-dependent rickets type 2.
Reduced sun exposure, prolonged vomiting and diarrhea, together with dietary deficiencies of calcium, magnesium and phosphorus, can favor the onset of rickets. Not surprisingly, it is a rather common disease in developing countries, where poor hygiene conditions add to malnutrition.
Symptoms

Vitamin D synthesis
To better understand the etiology of the various forms of rickets, it is necessary to know the metabolism of vitamin D within the human organism:
- Vitamin D3 or cholecalciferol is produced for 90% in the skin from cholesterol, through the action of solar UVA rays, and only 10% is introduced with the diet.
- Vitamin D3 synthesized in the skin must undergo some transformations before being active. The first occurs in the liver, where it undergoes a first hydroxylation in position 25 by a hepatic 25-hydroxylase. The product of this hydroxylation is therefore a 25-OH-D3.
- 25-OH-vitamin D3 is still devoid of biological activity; to acquire it it must be further hydroxylated in position 1 in the kidney, where a "renal alpha hydroxylase intervenes which transforms it into 1,25- (OH) 2-D3 or calcitriol, an active metabolite of vitamin D. Calcitriol causes increased intestinal absorption of calcium and the mobilization of calcium and phosphates in bone. The result is an increase in calcium (calcium concentration in the blood).
Types of Rickets
- The most frequent deficiency rickets is that of vit D; the insufficiency of calciferol induces the reduction of intestinal absorption of calcium, consequently hypocalcemia stimulates the production of parathyroid hormone, which reduces the renal excretion of the same mineral and stimulates its mobilization from the bones, reducing its mineralization.
- Hepatic osteodystrophy is, as the term itself implies, a "skeletal alteration induced by a pathology that compromises the liver; among these, the most common are biliary cirrhosis and biliary arthrosis. As liver activity is compromised, low levels of both 25-OH-D3 and 1,25- (OH) 2-D3 are recorded.
Rickets from anticonvulsant therapy, on the other hand, is attributable to the use of drugs such as barbiturates which, in 10-30% of cases, generate problems related to skeletal deformation. - Familial hypophosphatemic rickets is an autosomal dominant genetically transmitted disease; the incidence is estimated between 1 / 10,000 and 1 / 1,000,000 but the most likely ratio seems to be 1 / 20,000.
Vitamin D-dependent rickets type 1 is induced by a mutation in the gene encoding renal alpha-hydroxylase, resulting in low levels of 1,25- (OH) 2-D3.
Renal osteodystrophy is due to the reduction of renal function typical of chronic renal insufficiency which often determines the onset of secondary hyperparathyroidism [hyperphosphatemia hypocalcemia and reduced synthesis of 1,25- (OH) 2-D3 present in low concentrations due to of poor renal activity].
The rickets due to tubulopathies is attributable to pathologies such as Fanconi's syndrome, type 1 tyrosinemia and tubular acidosis.
Oncogenic rickets, on the other hand, is related to some forms of neoplasia (usually benign) of mesenchymal origin that generate hypophosphataemia due to reduced intestinal reabsorption of phosphate added to low levels of 1,25 (OH) 2. - Type 2 rickets is caused by tissue resistance of the target organs to 1,25- (OH) 2-D3; unlike type 1 rickets, where its levels are particularly low, in patients with type 2 rickets l "1,25- (OH) 2-D3 is very high
With regard to chronic intestinal malabsorption rickets, it is a secondary complication to other conditions such as celiac disease, cystic fibrosis and intestinal resections; these are responsible for both calcium malabsorption and vitamin D.
In both cases, low levels of both 25-OH-D3 and 1,25- (OH) 2-D3 are recorded.

- vit. D [both 25 (OH) and 1.25 (OH) 2]
- calcemia
- phosphatemia
but to do this, in the forms of secondary rickets it is necessary to undertake a therapy useful for the resolution of the primary disease. Genetic alterations do not fall into this category and, to reduce complications, it is necessary to increase the intake of vitamin D above the normal recommended doses.
Bibliography:
- Pediatric manual - M. A. Castello - Piccin - chap5 - page 152: 158.