Septic arthritis: introduction
As analyzed in the previous discussion, "septic arthritis is a" painful infection of the joints, the cause of which resides, more often, in bacterial insults and, more rarely, in viral and fungal attacks. Septic arthritis causes extremely painful symptoms, associated with redness, swelling and burning sensation; after analyzing in more detail the symptoms that characterize septic arthritis, we will analyze the diagnostic strategies and therapies available for the treatment of the disease.

Symptoms
Normally, septic arthritis does not go unnoticed, since it often begins with painful symptoms in the involved joint. In addition to the omnipresent joint pain, which tends to worsen with movement, the patient often complains of high fever (even 40 ° C), joint swelling, acute synovitis, vasculitis and a particular burning sensation at the level of the site involved. In children in particular , septic arthritis can also cause mood swings (irritability), general malaise, loss of appetite and tachycardia.
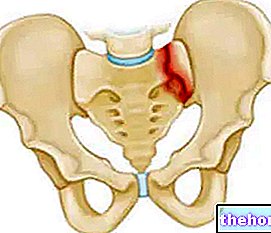
Some patients develop septic arthritis in joints such as the sternoclavicular, the acromion-clavicle (clavicle and shoulder blade) and the sterno-costal: in these cases, the pain can spread and also involve the chest. When septic arthritis affects the sacroiliac area, it is very likely that the patient feels acute pain in the buttocks, hips or anterior part of the thigh.
Infantile septic arthritis tends to manifest itself more often in the hips, while in adults the joints of the legs and arms (therefore also the knee, elbow, wrist and ankle) are the most affected; head, neck and other joints can also be affected.
When the infection is not stopped and eradicated in time, the damage could also be permanent (functional impotence) and, in some cases, so severe as to cause the death of the patient who is affected by it.
Diagnosis
To ascertain the diagnosis of a clinical case of septic arthritis, the presence of pus in the joint and the rapid destruction of the cartilage must be observed.
A patient already being treated for arthritis, who therefore takes specific drugs, may not perceive the typical pain that accompanies septic arthritis: the drugs, in fact, mask the alarming symptoms that septic arthritis normally sends.
The most commonly used diagnostic tests include "aspiration of joint fluid for cell count (analysis of a sample of synovial fluid taken with a needle directly inside the joint), Gram stain, blood tests," blood culture and radiography (test of imaging).
By examining necrotic tissues taken from a patient with septic arthritis in the laboratory, it is possible to observe some interesting findings:
- Inflammatory infiltrate consisting mainly of polymorphonuclear neutrophils
- Exudate with a serous, clear / cloudy or purulent appearance
- Thickening of the joint capsule and production of intraarticular fibrous elements (responsible for impaired mobility)
- Neutrophilic leukocytosis:> 7500 leukocytes / mm3, of which over 85% are neutrophils
- Very high ESR (erythrocyte sedimentation rate, in reference to the erythrocyte sedimentation rate): the high ESR value indicates an "inflammation in progress
- Very high C reactive protein
Among the molecular investigations, PCR should not be forgotten (Polymerase Chain Reaction), essential for ascertaining the presence of bacterial DNA in synovial fluid and joint tissue: this diagnostic technique is useful for identifying pathogens that are difficult to cultivate.
From the radiological examination, however, not much information is obtained, since only the volumetric increase of the para-articular soft tissues and the opacity of the same can possibly be observed.
Through the "CT exam (computed tomography) and MRI (magnetic resonance imaging) it is possible to obtain a more accurate morphological evaluation of the pathology: CT, in fact, better defines complex joints, proving to be a very useful test that acts as a guide for fine needle aspiration. The MRI test, being very sensitive , allows for a quick diagnosis and is much more specific than conventional radiology.
In the event that it is not possible to isolate any pathogen, it is recommended to evaluate the quantity of neutrophils in the synovial fluid: when the count of these cells is greater than 20,000-30,000 units / mm3, the diagnosis of septic arthritis is very probable.
Useful data to ascertain septic arthritis from a sample of synovial fluid: chemical-physical examination
Appearance → opaque
Color → greenish-yellow
White blood cells →> 100,000 units per mm3
Glucose → friable
Mucin → positive (80%)
Neutrophils →> 75%
Viscosity → variable
Volume →> 3.5
Prognosis
The course of the infection is heavily influenced by numerous factors:
- Virulence of the pathogen
- Early onset of therapy
- Guest response
- Efficiency of the host's immune system
- Age of the patient
- Location of the pathogen (number of affected joints)
It is believed that 5-10% of aseptic arthritis due to gram negative and S. aureusthe prognosis is poor, despite adequate and prompt therapy; septic arthritis is highly disabling (leaves permanent lesions) in 25-50% of cases.
Care
Even if only if septic arthritis is suspected, it is recommended to proceed as soon as possible with aggressive treatment in a hospital setting, in order to subject the patient to rapid tests to begin treatment immediately. During therapy, even if immobilization of the limb is not always necessary, it is recommended to avoid weight loading.
Drug therapy is subject to the type of etiopathological agent involved, identified only after culture of aspirated synovial fluid or blood culture.
Generally, the therapy consists in the administration of antibiotics (in case of bacterial septic arthritis) to be taken intravenously for three weeks; after this first treatment, it is recommended to proceed with oral therapy for another 2 weeks.
In addition to antibiotic therapy, the patient with septic arthritis is generally also subjected to drainage of the joint, often performed with needle aspiration; the drainage can also be surgical but, in this case, it is preferable to undergo this operation only for patients who present evident involvement of the axial joints (such as shoulder, hip and sternoclavicular joint) and in case of failure to respond to antibiotic therapy. Drainage gives the patient immediate relief and decreases joint pressure.
Remember that timely therapy for the treatment of septic arthritis can often prevent the onset of irreversible damage.
Other articles on "Septic Arthritis - Symptoms, Diagnosis, Treatment"
- Septic arthritis
- Septic Arthritis - Drugs to Treat Septic Arthritis