The studies published on the subject agree on the fact that the problem is endemic, it affects in practice, at least once in a lifetime, almost the entire population.
Read also: The Best Postural Correctors
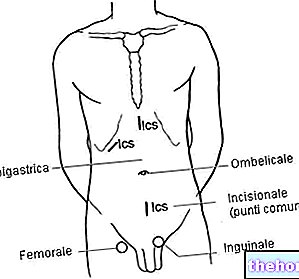
if the pain also affects the lower limb.For back pain we mean the painful picture that affects the entire area of the dorsal vertebrae, therefore from D12 to D1. a set of causes, it is therefore rare that it originates from a single structure. This confirms the fact that the individual must be analyzed in a global way, because the problems of the human body cannot be cataloged by sectors with watertight compartments, as unfortunately is doing official medicine.
By neck pain, on the other hand, we mean the problems related to the cervical spine. Which can be simple limitations of movement of rotation and inclination, or painful pictures resulting from cervical hernias or osteoarthritis.
Given the high percentage of people affected by back pain, the social costs that the problem causes are enormous.
The studies published in the literature are numerous and investigate the problem in all its facets: from the point of view of employment, sport, surgery, rehabilitation, etc. When it comes to back pain, numerous aspects must be taken into consideration, both of an anatomical-functional type and of a subjective type, so much so that it is very difficult to codify the problem in a few diagnostic categories.
The choice of treatment responds to many variables, which may be related to the type of pathology, the type of equipment available, the state of inflammation of the affected tract, etc.
Before proceeding to analyze the various types of treatment that I personally prefer to solve the problems of back pain, I would like to recall how the human body works, because it is itself that conditions the method used to solve painful problems and it is to it that the the operator's work must be adapted.
How does the human body work?
The human body is an articulated structure that is passively, actively and autonomously adaptable to various conditions. The mechanical structure is made up of rigid (bones), elastic-dynamic sealing elements (ligaments and bands), and dynamic (muscles); all correlated to form a complex biodynamic system.
The structures of the human body obey the laws of physics, such as those of static and dynamic equilibrium, of levers and fluids. Since the body structure is adaptable, we will have control systems that guarantee that this adaptability does not exceed certain limits, beyond which it does not it is more possible to compensate.
The main control systems are: the ophthalmic system, the vestibular system, the proprioceptive system and the exteroceptive system. Within these systems we find the motor engram, the kinetic chains, the attitudes, the positions and the psycho-physical experience of each individual.
Kinetic chains
Kinetic chains are the muscular systems through which our posture is articulated and modified.Physics states that a kinetic chain is a system composed of rigid segments, joined by moving junctions called joints. Our body is composed of many kinetic chains, the segments are represented by the bones while the joints represent the joints. Muscles are the "engine" of the kinetic chain. This engineering-like definition, however, is not fully applicable in the physiology of human movement because the muscular apparatus cannot be compared to a rigid mechanical system, but is to be considered as flexible and plastic.
The main kinetic chains to be taken into consideration for the treatment of back pain are: the posterior kinetic chain, the diaphragmatic kinetic chain, the transverse kinetic chains.
Diaphragm
The diaphragm plays a key role in back pain, it is an uneven and asymmetrical muscle that separates the chest from the abdomen.
It is the main muscle related to breathing. Its shape resembles that of a dome and is formed by a central tendon part, commonly called the "phrenic center", and a vertebral muscle part (costal and sternal). The first consists of two voluminous bundles of fibers: respectively the right pillar which fits on the L1-L2 and L2-L3 and sometimes L4 intervertebral discs, and the left pillar which fits on the L1-L2 and L2-L3 discs. The costal part originates on the inner face of the last six ribs and on the aponeuritic arches that join the apexes of the 10th, 11th and 12th ribs and which are inserted on the phrenic nerve. The sternal portion is made up of two muscle bundles deriving from the posterior aspect of the typhoid process, which always end on the phrenic center.
When an inhalation is triggered, the diaphragm contracts and its dome is lowered until it finds the resistance of the viscera and the suspensory tendon of the diaphragm. This triggers a depression inside the chest box and therefore the entry of air into it. Conversely, when the diaphragm relaxes and rises upwards, the expiratory mechanism is triggered.
The retraction of this muscle, which can be triggered for reasons of stress, psycho-physical trauma, asthma, etc. it forces the diaphragm to an always slowed exhalation and to an act of forced and prolonged inhalation.
The retraction of this muscle can trigger many pathologies. Once contracted, in fact, the muscle exerts a coacting force between origin and insertion causing a compression of the lumbar vertebrae which can lead to lumbago, discopathies and disc protusions. It can also be the precursor to stomach problems such as hiatal hernia, where the stomach escapes upward to escape the depression inflicted on it by the diaphragm, giving rise to a stomach undertow. Finally, the close contact between the psoas and the diaphragm can lead to a contractile process of the psoas itself which is a hyperlordifying of the spine.
However, we must not forget that not using the diaphragm properly triggers an overuse of the accessory musculature at rest consisting of: sternocleidomastoid, pectoral minor, subclavian, trapezius, scapula elevator, great dentate, great dorsal and erectors of the trunk. These hyperactivated muscles will in turn undergo retraction, therefore decompensation, causing possible neck pain, problems with the rotator cuff, limitation of movements, etc.
Correlation between psyche and posture
Psyche and posture are therefore linked; the thread that unites these two elements is often the diaphragm, but this is a complex, sometimes chaotic topic of posture, both under the diagnostic aspect (we often tend to forget or not talk about the events that caused stress or trauma to our organism, therefore these events will hardly come out during the anamnesis) than under the re-educational-therapeutic aspect. It is also true that the topic is so important and integrated into the system that it cannot be ignored and in some cases it is difficult to not to say impossible, to identify how much the postural action conditions a psychological component and vice versa.
. First of all, sporadic back pain should not be underestimated, as it informs us that we have an alarm bell in place. tears, contractures, etc.The anamnesis will be carried out carefully to understand the daily habits, to learn the experience of the client in question and the events that led to the emergence of the pain. It is also important to know how the moment of birth took place, if it was breastfed or used a bottle etc. In short, nothing should be left out.
Observe the patient-client is a must, slightly broken teeth, asymmetrical dental arches, tight jaw, evident dental fillings with harmful amalgam, glasses that are not perfectly symmetrical, head tilted or rotated in an anomalous or asymmetrical way, shoulders at different heights or internally rotated , asymmetrical triangles of size, how it breathes, how it positions itself on the chair and standing up how it distributes loads, valgus or varus knee, abnormal wear of shoes, etc.
After the anamnesis it will be necessary to perform a postural analysis with adequate tests. For completeness, albeit in a synthetic way, I report a series of tests to be performed on the subject: anterior bending test with evaluation of the symmetry of the pelvis, we can help with a mason's bubble to have a better overview; head rotation test; head tilt test; trunk lateral tilt test; palpation of the mandibular and hyoid muscles; palpation of the dorsal and trapezius muscles, appreciating the presence or absence of contractures or asymmetries; evaluation of the sacroiliac and piriformis; evaluation of the elasticity of the hamstring muscles, of the rectus femoris, ileo-psoas and rotator muscles of the femurs; adductor evaluation; assessment of the length of the lower limbs; Romberg test; Fukuda test; De Cyon test; search for nystagmus; Cover test; TMJ examination; examination on the stabilometric platform.
The postural re-education protocol will be performed taking into account these assessments, the proprioception training must not be forgotten as it plays a fundamental role in the positioning of one's body and body segments in space. The postural re-education must start from a general rebalancing , then stretching the muscles and then toning them in a balanced and proportionate way. Of course there are different schools of thought about how to act in the stretching of the muscles, personally I believe that a global decompensated stretching is the right way to act. It is not correct to follow trends when the well-being and health of the person is at stake, it is necessary to use methods supported by scientific studies that demonstrate their effective effectiveness.
After a global decompensated stretching session it is more than appropriate to perform a massage session that further relaxes the patient and in cases where you are faced with an important inflammation you can apply kinesiological taping which will perform a "decontracting, draining action. and proprioceptive on the musculature.