Peptic ulcer is a disease of considerable social importance. From the data currently available it appears that in Western countries 2% of the population has an active ulcer, while 6-15% presented clinical manifestations compatible with the presence of of gastric or duodenal ulcer. Men are affected more frequently than women, with a ratio of 3: 1. The duodenal localization is the most frequent, except in Japanese statistics, in which gastric ulcer prevails. 5-15% of patients present simultaneously gastric and duodenal ulcer. In men the onset of peptic ulcer is rare before the age of 20 , but its incidence grows over the following decades until it reaches a maximum peak at the age of 50. The onset of ulcer in women is infrequent in the pre-menopausal age; this suggests a possible protective role exerted by hormones. The incidence of peptic ulcer, particularly of the duodenal ulcer, has been decreasing in the last 30 years, probably in relation to the discovery of the factors that cause it and their relative elimination.

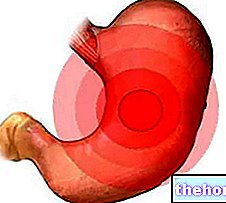
The peptic ulcer is a localized lesion that affects the mucosa of the digestive system exposed to the action of the secreted stomach acid.The most frequent localization of the ulcer is in the stomach and duodenum, but it can also appear in the esophagus, in cases of acid or alkaline reflux from the stomach to the esophagus itself, in the jejunum, after surgery that has removed the lower half. of the stomach and duodenum, in Zollinger-Ellison syndrome (an often familiar tumor of the endocrine system, and sometimes also in Mekel's diverticulum (a diverticulum of the small intestine), due to the presence of gastric mucosa when, normally, this should not be there.
The gastric secretion of hydrochloric acid and pepsin plays a fundamental role in the onset of the ulcer; in fact, it has been shown that the peptic ulcer does not arise in the case of achlorhydria (lack of acid secretion). The gastric and duodenal mucous membranes, in normal conditions, are very resistant to the action of the peptic acid secretion; the onset of ulcer in the stomach and duodenum is therefore considered the result of an imbalance between the aggressive factors for the mucosa (acid and pepsin, gastric-injuring substances, bacteria, etc.) and the defensive ones (secretion of mucus and bicarbonate, blood flow mucosa, cell turnover), which participate in the formation of the so-called "mucous barrier". The mucosa of the other tracts of the digestive system is instead particularly sensitive to gastric secretions; acid reflux in the lower portion of the esophagus in subjects with incontinence of the cardia (the valve that separates the esophagus from the stomach), or the passage of acid chyme in fasting following surgical removal of a portion of the stomach and duodenum, they can in fact induce the onset of peptic ulcers. However, these last two forms have a very low incidence, therefore, the term peptic ulcer commonly indicates the gastro-duodenal ulcer disease, which represents 98% of the entire ulcer disease.
If we observe a small portion of tissue that constitutes the peptic ulcer under the optical microscope, we can appreciate a lesion of the mucosa and submucosa, almost always solitary, which can deepen into the gastric or duodenal wall beyond the muscularis mucosae, reaching and often exceeding the muscular tunic This distinguishes ulcers from simple mucous erosions, characterized by rapid and complete resolution, because they are limited to the epithelium of the mucosa. In some cases, however, mucosal erosion, rather than a distinct entity, represents a simple initial stage of the onset of the ulcer. The gastric ulcer and the duodenal ulcer are in many respects different from each other and are therefore illustrated separately.
Laboratory and instrumental investigations
The use of laboratory tests and instrumental investigations is essential to ascertain the diagnosis, formulate the prognosis and guide the therapeutic conduct of stomach and duodenal diseases. The most important methods for the study of gastro-duodenal diseases are:
- L"digestive endoscopy, with the methods associated with it (endoscopic biopsy, chromoendoscopy, operative endoscopy, endoscopic ultrasound). it is certainly the most frequently used examination, due to the fact that it requires short execution times and uses a simple technique. Moreover, in emergency conditions it can also be performed in the operating room.
- L"radiological examination of the first tract of the digestive tract with radio-opaque meal;
- there evaluation of gastric secretory activity;
- the gastrinemia dosage.
The research of the occult blood in faeces it is a non-specific examination but useful in the initial "diagnostic" phase (screening); the positivity of the test indicates a small but constant blood bleeding (oozing) in the digestive tract. The stomach and duodenum are among the most frequent sites of bleeding.
Ultrasound and CT of the abdomen second choice tests are almost always to be considered, useful for defining the nature of new formations that cause compression from the outside on the stomach and duodenum and for evaluating the possible involvement of other abdominal organs by a primitive gastro-duodenal pathology, such as frequent liver metastases caused by gastric cancer.
L"selective arteriography of the celiac trunk and superior mesenteric artery it can sometimes be used to identify the site of bleeding in the case of ongoing digestive bleeding; it is a rarely used radiological examination, which has been replaced in most cases by endoscopy.
Other articles on "Ulcer"
- Grastic ulcer
- Duodenal ulcer
- Peptic ulcer therapy
- Medicines to Treat Ulcer
- Ulcer: herbal medicine and natural remedies