
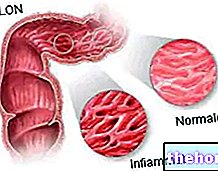
Intestinal adhesions as a possible cause of intestinal obstruction: these are bundles of fibrous tissue (internal scars) that form as a result of trauma, inflammatory processes or surgery
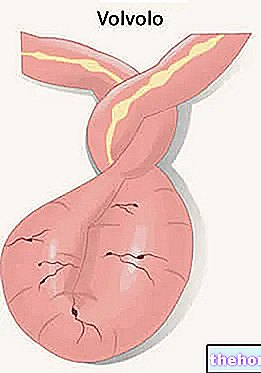
First of all, two large families of intestinal obstructions are distinguished: those on a functional basis, due to the arrest of peristalsis due to paralysis of the enteric muscles (paralytic or adynamic ileus), and those on a mechanical basis, due to the presence of a physical obstacle (mechanical ileus) .
The characteristic symptom of intestinal obstruction is abdominal pain, often accompanied by a sense of bloating, nausea and vomiting.
In the absence of treatment, intestinal obstruction can lead to necrosis of the enteric portion affected by the occlusion, with the risk of intestinal wall perforation, peritonitis, septicemia and shock. However, prompt medical attention is generally effective in preventing these unpleasant and dangerous occurrences.
The signs and symptoms typically associated with intestinal obstruction include cramping and intermittent abdominal pain (except in cases of strangulation, where the pain is continuous), nausea, vomiting (the earlier the higher the location of the lesion), constipation (closing of the alvus to stool and gas) with inability to expel intestinal contents and consequent distension of the abdomen. paralytic ileus (silence of the abdomen) or advanced mechanical ileus (when peristalsis ceases "surrendering" to the "obstruction). Also noteworthy is the hydro-electrolytic imbalance due to the lack of reabsorption of digestive juices (every day they are secreted and 7-8 liters of digestive juices are poured into the intestine, in addition to liquids introduced from the outside; obviously, failure to absorb these liquids causes dehydration e, hypovolaemia and hypotension).
congenital, atresias, Crohn's disease, diverticulitis, laparoceles, fecalomas, foreign bodies, parasites and gallstones.
Among the possible causes of intestinal obstruction linked to paralysis of the enteric muscles (paralytic or adynamic ileus) we remember: abdominal or pelvic surgery, infections and peritonitis, trauma of the abdomen, some drugs (opiates, neuroplegics, muscle relaxants) and diseases of the muscles or of the nervous system such as Parkinson's disease.
The early treatment of intestinal obstruction is essential for the prevention of complications, essentially represented by necrotic phenomena of the intestinal tract affected by the obstruction, with possible perforation of its walls, diffuse peritonitis, sepsis and shock. Of course, the treatment of intestinal obstruction depends on the causes that generated it; common, if the conditions so require, is the need to hospitalize the patient to monitor the conditions and vital parameters, and correct dehydration. The excess of gastric fluids can be absorbed through a nasogastric tube, while the application of the catheter ensures urine drainage and the possibility of rapid examination of the same. Normally the patient is kept on an absolute fast and fed intravenously; antibiotic prophylaxis is often useful. This phase, lasting a few hours, aims to stabilize the condition of the patient affected by intestinal obstruction and to prepare him in the best possible way to face any surgery.
When necessary, as occurs in complete mechanical obstructions, major surgery is required to resolve the blockage or eliminate the necrotic parts of the intestine. Paralytic ileus, on the other hand, generally tends towards spontaneous resolution within a few days; if doctors deem it appropriate, healing can in any case be favored or accelerated by the administration of drugs (such as prostigmine) which increase the contractility of the abdominal muscles, favoring the advancement of the enteric content blocked by intestinal obstruction.




















-nelle-carni-di-maiale.jpg)




