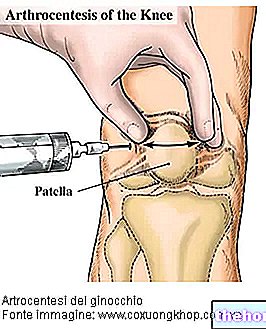
Cortisone infiltrations involve injecting the drug directly into the joint affected by inflammatory processes. The rationale for such a treatment is to be found in the therapeutic effects of cortisone and in the possibility of limiting its side effects, certainly greater when the drug is taken by mouth.

The therapeutic scheme varies according to the type of pathology and its severity: the "standard approach involves one" infiltration per week for a variable number of times (from three to five), but due to the possible side effects some doctors recommend not exceed 3-4 infiltrations per year, separating them by at least a month.
The powerful anti-inflammatory and immunosuppressive effect of cortisone helps to relieve pain and joint effusions in the acute phase of the disease.
,- even at the intra-articular level, the abuse of these drugs can cause serious consequences.
Chronic Side Effects
An excessive number of cortisone infiltrations can weaken tendons, ligaments, bones and other structures that participate in the joint. Furthermore, the small amount of drug that enters the circulation can be important for some categories of patients.
Acute Side Effects
If carried out in compliance with the rules of asepsis (hair removal, thorough cleansing and disinfection of the skin, replacement of the needle after aspiration of the drug), the infiltration of cortisone generally does not cause any significant local effect. the risk of inflammatory reaction stands out, with local pain and redness that tend to resolve within 24 hours, spontaneously or through the aid of non-steroidal anti-inflammatory drugs. Skin atrophy and depigmentation of the treated area are the possible consequence of extravasation of cortisone through the needle path into the surrounding skin.
with warfarin (Coumadin) or acenocoumarol (Sintrom): risk of bleeding inside the jointFor this reason it is good to limit the use of cortisone infiltrations to the acute phases of arthropathies, when pain and inflammation are important and severely limit joint mobility. After this phase, it is preferable to resort to specific infiltrations of hyaluronic acid which have demonstrated an antalgic efficacy comparable to that of intra-articular injections of cortisone. Furthermore, hyaluronic acid is a natural component of the joint and is free from important effects. collateral ascribed to prolonged cortisone therapies The infiltrations of sodium hyaluronate are preferable to those of cortisone especially in the case of arthrosis.