when diuresis falls below 400-500 ml in 24 hours, while the term polyuria is used to indicate a production of urine above 2000 - 2500 ml (2 - 2.5 liters) per day.
These alterations in diuresis can be benign or the result of particular pathologies; polyuria, for example, is among other things a characteristic symptom of the various forms of diabetes, while oliguria is typical of nephritis, renal colic and all diseases that cause dehydration (such as those that result in diarrhea, for example viral gastroenteritis).
Anuria
In anuria, diuresis drops below 100 ml in 24 hours; we are therefore talking about a pathological condition characterized by severe renal impairment.
Nocturia and Other Alterations
In addition to quantitative alterations, there are other forms. Nocturia, for example, leads the patient to urinate especially at night; this is a typical problem of patients with heart failure, caused by the nocturnal reabsorption of edema. This alteration of diuresis is also typical of men with prostate problems, in which it is often accompanied by rather annoying disorders, such as burning or pain during urination, and the sense of incomplete emptying of the bladder, with the consequent need to urinate often .
We recall that urination represents the physiological act that leads to the expulsion of the urine contained in the bladder to the outside.
which reaches the kidneys, equal to about 700 ml per minute.Glomerular filtrate (amount of plasma filtered in the unit of time)
The glomeruli filter about 80% of the blood that reaches the kidney, so roughly 150 ml of plasma per minute for a total of around 180 liters per day. This liquid is called preurin and under normal conditions it contains all the substances present in the blood, with the exception of cells (white, red blood cells, platelets, etc.) and larger plasma proteins.
Tubular reabsorption
Without reabsorption of fluids by the kidney, diuresis would be 180 L per day. Of course, the body cannot afford to waste such a precious element, so it reabsorbs the vast majority of the glomerular filtrate and the nutrients it contains. 90% of this reabsorption is independent of hormones (occurs for osmotic reasons, linked to the reabsorption of sodium), while the reabsorbable percentage of the remaining 18 liters is regulated at the endocrine level. In particular, the diuresis regulatory hormone par excellence is known as vasopressin, ADH or antidiuretic hormone. As the name suggests, ADH reduces diuresis. Not surprisingly, in its absence we speak of diabetes insipidus, a disease that if not treated can be accompanied by the conspicuous emission of urine, up to 18 liters / day in cases of total deficiency of the hormone or failure to respond to its action.
For what has been said, the secretion of vasopressin increases in conditions of dehydration, since in such circumstances it is necessary to retain as much water as possible in the body. Urinary losses can and should instead increase when the individual drinks excessively and in this case the ADH secretion decreases. The directors of this fine regulation mechanism are the hypothalamic cells of the thirst center, which act as osmoreceptors; as such, they are able to pick up changes in the osmolarity of the blood (that is, if this is more or less concentrated), inducing or inhibiting the secretion of vasopressin at the level of the posterior pituitary (neurohypophysis) as needed.
Other hormones
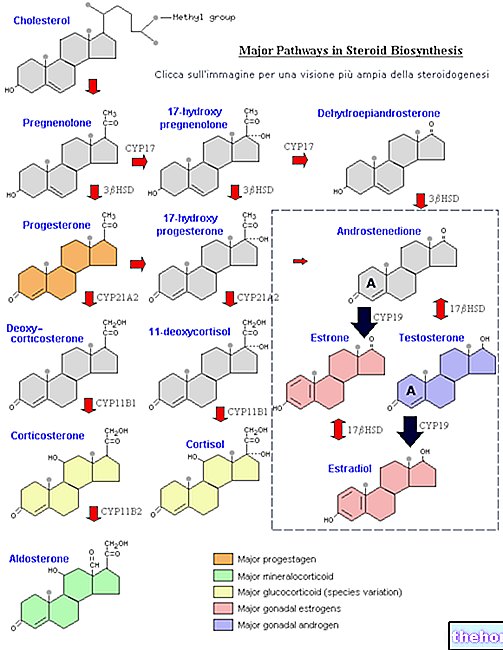
Another very important hormone in the regulation of diuresis is "aldosterone. Produced by the adrenal gland, this steroid hormone (derived from cholesterol) increases the reabsorption of sodium in the distal tubule and in the collecting duct, while accelerating the elimination of potassium and hydrogen ions. Basically, it therefore has an inhibiting effect on diuresis, also mediated by its stimulation on the release of the antidiuretic hormone.
Among the hormones with a diuretic effect we remember the atrial natriuretic peptide; it is a peptide secreted by specialized cells of the myocardium following an excessive increase in blood volume (high blood pressure). Since the pressure increases as the volume of blood increases, in such conditions it is necessary to deprive it of part of its liquid component; this result is obtained by simply increasing the diuresis.
Most of the diuretic drugs, as well as some foods in common use (those containing xanthines, such as coffee, tea, cocoa and derivatives), stimulate diuresis by acting not so much as hormones, but rather as inhibitors of the reabsorption of minerals, which for osmotic reasons they recall water by increasing diuresis.









.jpg)











