The main products deriving from digestion and intestinal absorption of carbohydrates are glucose, galactose and fructose. Through the mesenteric vein and the portal vein these sugars reach the hepatic capillaries, where they are retained in large quantities.
It is precisely in the liver that galactose and fructose are converted into glucose, which is, in practice, the only sugar present in the bloodstream. The term glycaemia is used to indicate its concentration in the blood. In a healthy person this parameter fluctuates, when fasting, between 80 and 100 mg / dl. For the individual to be healthy, it is essential that blood sugar remains relatively constant throughout the 24 hours.

The importance of circulating glucose in the blood is linked to the inability of neurons to draw energy from other energy substrates, such as fats and amino acids. Signs of brain distress already occur for glycemic values below 60 mg / dl and are responsible for the typical symptoms previously illustrated.
When the blood sugar increases excessively, once the threshold value of 180 mg / dl is reached, the body begins to lose glucose in the urine (glycosuria). This, which at first glance might seem an effective defense mechanism, is actually a dangerous phenomenon. , because for osmotic reasons the urine containing glucose attracts a lot of water, with consequent dehydration of the body.
Under physiological conditions, glycosuria is equal to 0.
When sugars absorbed from the intestine enter the liver through the portal vein, they can undergo different fates.
First of all, they can be degraded by the liver cells to draw the energy necessary to meet the metabolic demands of the hepatocytes.
Glucose can also be converted into glycogen, which is our body's sugar reserve. A certain amount can also be transformed into triglycerides.
The fate of sugars is heavily conditioned by the nutritional status of the subject.
-In response to a meal that is particularly rich in carbohydrates, the liver tries to bring blood sugar back to normal:
1) converting its metabolism, normally based on the oxidation of fats, with the aim of consuming mainly sugars
2) increasing glycogen stores in hepatocytes
3) promoting the conversion of glucose into fatty acids
PLEASE NOTE: glycogen, which is reduced in the individual glucose monomers during fasting, can be stored at a maximum in quantities equal to 5-6% of the liver mass (about 100 grams). Once these supplies are saturated, the liver is forced to convert excess sugars into reserve adipose tissue. For this reason, a diet low in fat and rich in carbohydrates (pasta, bread, cereals and derivatives, sweets, etc.) is not effective in treating promote the reduction of body weight.
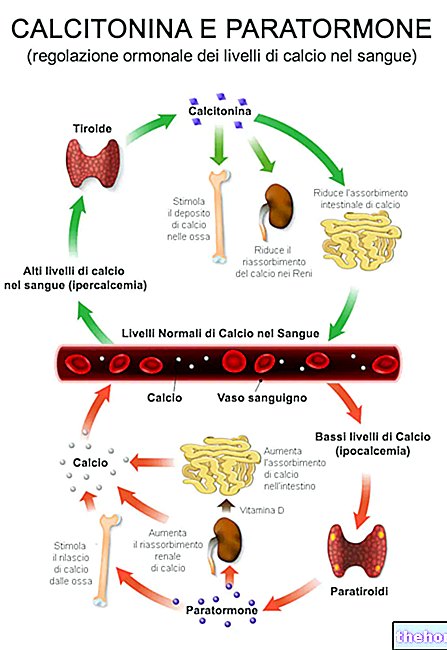
The liver also regulates blood sugar through the intervention of various hormones; the most known and influential are called, respectively, insulin and glucagon.
The regulating action on glycemic values is not entrusted only to the liver; in the same way, insulin does not act only on hepatocytes but influences the metabolism of various tissues. In the muscle, for example, this hormone favors the entry of glucose which, in addition to being degraded with glycolysis, is transformed into storage glycogen.
Insulin also acts at the level of adipose tissue, increasing the uptake of glucose and stimulating its deposit in the form of triglycerides.
CONTINUE: Carbohydrates and hypoglycemia "





.jpg)