Generality
Budd-Chiari syndrome is a rare set of signs and symptoms, triggered by total or partial occlusion of the hepatic veins. This occlusion can be caused by a venous thrombosis or external compression, although it must be remembered that in half of the cases it is idiopathic.

Figure: the hepatic veins are blood vessels that drain the de-oxygenated blood flowing from the liver, and pour it into the inferior vena cava. From the site: espondilitis.eu
Symptoms that characterize Budd-Chiari syndrome are different; the main ones are ascites, hepatomegaly, abdominal pain and jaundice. Symptoms can have a sudden onset (acute form) or gradual (chronic form).
Diagnosis is based on a physical examination followed by a series of more specific checks, such as CT or angiography.
The therapeutic treatment, which is used in most cases, is TIPS, a surgical procedure for the construction of an artificial canal that avoids venous blockage.
What is Budd-Chiari Syndrome?
Budd-Chiari syndrome is a disease caused by partial or total occlusion of the hepatic veins (blood vessels that drain and collect blood from the liver).
Occlusion can affect venous ducts of any size, from the smallest to the largest.
WHERE DO HEPATIC VEINS GATHER?
From the anatomical point of view, it should be remembered that the hepatic veins flow into the inferior vena cava; it is a large vessel designed to collect all the oxygen-poor blood coming from the subdiaphragmatic region of the body.
MAIN CONSEQUENCES OF BUDD-CHIARI SYNDROME
Due to hepatic venous occlusion, the blood cannot leave the liver, therefore causing the organ to enlarge (hepatomegaly). All this also has another consequence: it increases the blood pressure in the portal vein (the large venous vessel that collects blood from the intestine and transports it to the liver); this pathological process is called portal hypertension.
The onset of portal hypertension has several effects:
- Causes an abnormal dilation of the submucosal veins of the esophagus (esophageal varices)
- It damages the cells that make up the liver tissue
- It gives rise to ascites, which is a pathological collection of fluids in the abdominal cavity. The exact point where the liquid accumulates is between the two sheets that make up the peritoneum: this space is called the peritoneal cavity.
CLASSIFICATION OF BUDD-CHIARI SYNDROME
Budd-Chiari syndrome can be acute / fulminant (20% of cases) or chronic (80% of cases).
EPIDEMIOLOGY
Budd-Chiari syndrome is very rare; according to medical statistics, in fact, it affects one person in every million individuals. It does not prefer a particular sex but is more common between the ages of 20 and 40.
Causes
In at least half of the cases, Budd-Chiari syndrome occurs without a definite cause (idiopathic Budd-Chiari syndrome).
When the causes are identifiable, the disease may instead depend on thrombosis affecting the hepatic veins (primary Budd-Chiari syndrome) or external compression of the same veins (secondary Budd-Chiari syndrome).
IDIOPATHIC BUDD-CHIARI SYNDROME
In medicine, a disease is called idiopathic when it arises for no identifiable reason.
PRIMARY BUDD-CHIARI SYNDROME
Thrombosis is a pathological process characterized by the formation of one or more blood clots (called thrombus), inside the blood vessels (we speak of venous thrombosis if it occurs in the veins, and arterial thrombosis if it occurs in the arteries).
The presence of even a single thrombus can obstruct the lumen of the vessel and block the flow of blood downstream of the clot.
A thrombosis of the hepatic veins can occur due to:
- True polycythemia
- Antiphospholipid syndrome
- A complicated pregnancy
- A genetic tendency to thrombosis, due to deficiency or defect of some fundamental elements of the coagulation process (protein C, protein S, factor V of Leiden, prothrombin, antithrombin, etc.).
- Septicemia
- Sickle cell anemia
- Use of the contraceptive pill
- Paroxysmal nocturnal hemoglobinuria
- Anticoagulant lupus
SECONDARY BUDD-CHIARI SYNDROME
Secondary Budd-Chiari syndrome can arise as a result of:
- Phlebitis
- Autoimmune diseases such as Behçet's disease
- Tumors in organs or tissues adjacent to the liver (for example, renal cell carcinoma, hepatocellular carcinoma, or adrenal carcinoma)
- Trauma
- Presence, at birth, of a kind of membrane (membranous obliteration) that blocks the inferior vena cava. This anomaly is particularly widespread in Asia and in some African states (for example South Africa).
- Leiomyosarcoma
Symptoms and Complications
The classic symptoms and signs of Budd-Chiari syndrome are abdominal pain, ascites, jaundice and hepatomegaly.
In some cases, patients may also have an elevated level of liver enzymes, splenomegaly (enlarged spleen), vomiting, haematemesis (vomiting blood), hepatic encephalopathy, leg edema, and diarrhea.
CHARACTERISTICS OF THE ACUTE AND CHRONIC FORMS
The acute form of Budd-Chiari syndrome is characterized by intense symptoms with rapid and sudden onset.
In some situations it is so serious that within a few hours or days it can lead to death, due to the onset of a condition of shock and hepatic coma (acute fulminant form).
Most common symptoms of the acute form
- Abdominal pain
- Hepatomegaly
- Vomiting and hematemesis
- Jaundice
- Splenomegaly
- Diarrhea
- Ascites
- Abdominal pain
- Ascites
- Hepatomegaly

Figure: Ascites. The collection of fluids that occurs during ascites swells the abdomen quite noticeably. From the site: dynamic.psu.ac.th
The chronic form, on the other hand, has a gradual onset and slow progression. Sometimes, some patients remain asymptomatic (that is, they have no symptoms) for several consecutive years.
COMPLICATIONS
In some people, Budd-Chiari syndrome can involve liver cirrhosis, which is the replacement of liver cells with functional scar tissue.
Due to liver cirrhosis, a condition of liver failure is established, which is incompatible with a normal life.
Diagnosis
The signs that lead a doctor to suspect Budd-Chiari syndrome are hepatomegaly, ascites, and high levels of liver enzymes, found in blood tests.
However, in order to resolve any doubts and discover the causes that caused the suspected signs and symptoms, the following diagnostic tests must be performed:
- Doppler ultrasound
- Nuclear magnetic resonance (MRI)
- CT scan (computed axial tomography)
- Liver biopsy. It is also important to rule out similar diseases (differential diagnosis), such as galactosemia and Reye's syndrome
- Angiography
Treatment
Therapy varies according to the causes and associated symptoms (type of symptoms, speed of onset of disorders, degree of intensity, etc.).
Patients with ascites and leg edema are prescribed diuretic drugs and a low-sodium diet.
Patients with thrombosis of the hepatic veins may be prescribed treatment with thrombolytic drugs (eg heparin).

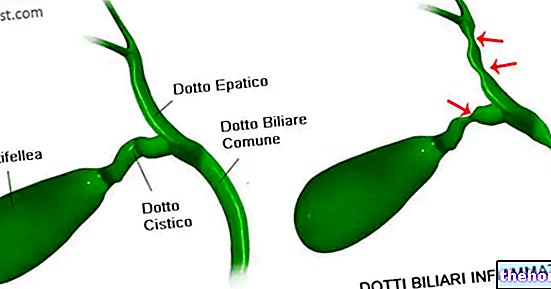
Figure: CT scan of an individual with Budd-Chiari syndrome. Arrows indicate venous occlusions. From the site: wikipedia.org
In almost all patients, surgery, known as TIPS, is required to construct an alternative passage to venous blood flow.
An "alternative to TIPS is represented by the" angioplasty operation, with which the narrowed or completely obstructed blood vessel (or blood vessels, if there are more than one) is dilated.
TIPS
The TIPS, or Shunt Transjugular intrahepatic portosystemic, involves the creation of an artificial canal (called shunt), which connects the portal vein with the hepatic vein; in this way it is possible to bypass the vascular occlusion.
The realization of the shunt, whose component material is introduced through the jugular, is a very complex procedure, which requires the use of a precise X-ray guide.
Risks of the intervention of TIPS: TIPS can result in (or worsen) hepatic encephalopathy.
WHAT TO DO IN CASE OF LIVER CIRRHOSIS?
In cases of liver cirrhosis, the most suitable treatment would be liver transplantation, a very delicate surgical operation that is not without possible complications.
Prognosis
Budd-Chiari syndrome tends to have a poor prognosis.
The chances of recovery, in fact, are few and are further reduced if the triggering causes are serious or if the therapy is late (i.e. it begins when the liver is already partially damaged).
According to some statistical research, thanks to adequate treatments 2/3 of individuals with Budd-Chiari syndrome live for about 10 years from the moment of diagnosis.