Generality
Hypertensive retinopathy is an eye disease that occurs in subjects with high systemic blood pressure values.

Healthy retina

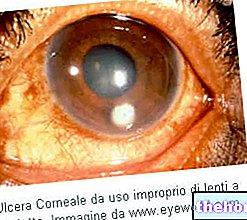
Retinal image of the left eye in a patient with chronic hypertension and dyslipidemia, with blurred vision; note the vascular tortuosity and arteriosclerotic changes.
At the ocular level, this condition negatively affects the retinal tissue, the choroid and the optic nerve, causing a wide spectrum of vascular damage.
Inside the retinal arterioles, the increase in pressure triggers vascular compensation mechanisms. Initially, the contraction of the elastic fibrils of the blood vessel wall occurs, which leads to a narrowing of the lumen of the same and an increase in tortuosity along their course.
However, when the pressure stress is excessive (hypertensive crisis) or protracted over time (chronic hypertension), these reactions are insufficient and stop. The result is a "structural alteration of the vascular wall, which undergoes exhaustion and becomes incontinent. Therefore, extravasations of liquids occur in the retinal tissue (exudates) and haemorrhages that can compromise the correct functionality of the retina.
In the advanced stages, when systemic arterial pressure has been elevated for years and is poorly controlled by proper therapy, edema, deposition of hard exudates around the fovea (macular star) and ischemic areas can develop.
In most cases, symptoms appear in the later stages of hypertensive retinopathy.
Fortunately, the involvement of the retinal circulation can be found during an eye examination by examining the fundus with the ophthalmoscope. Undergoing periodic check-ups can therefore contribute to the early diagnosis of "latent systemic hypertension and allows the initiation of adequate pharmacological treatment.
What is hypertension? Hypertension is the increase in systolic and / or diastolic blood pressure, over 140 mm of mercury (mmHg) for the maximum and 90 mmHg for the minimum. The natural evolution of untreated arterial hypertension involves the gradual and progressive onset of lesions in some target organs (heart, brain, eyes and kidneys).
Causes
Hypertensive retinopathy is an expression of the vascular damage induced by arterial hypertension at the ocular level. These changes are directly related to the duration and levels of the increase in blood pressure; in general, the effects on the retinal circulation are slow and progressive, but in the long run they can compromise the normal mechanism of vision.
An acute increase in blood pressure is characterized by a vasoconstriction of the retinal arteries, followed by haemorrhages of various sizes and exudative changes. If acute hypertensive retinopathy is very severe (hypertensive crisis), the optic disc becomes congested and may be raised due to papillary edema (or papilledema).
When the systemic hypertensive state is poorly controlled with correct therapy for a long period, however, point-like hemorrhages (called "flame") and retinal edema typically appear. In this form associated with chronic hypertension, the characteristics of arteriosclerotic retinopathy prevail (eg vascular tortuosity and compression at the level of the intersections between arterial and venous vessels).
With the further progression of hypertension at the retinal level, it is possible to find the deposition of hard exudates and the ischemic suffering of the retinal cells which, dying, are deposited in cottony nodules and drusen.
To consider: hypertension is a risk factor for other eye diseases, such as diabetic retinopathy and arterial and venous occlusions of the retina.
Symptoms
In the early stage, hypertensive retinopathy generally causes no symptoms.
However, in the advanced stages of the disease, vision can be blurred and images distorted. The retina, in fact, no longer nourished and oxygenated sufficiently, undergoes degeneration.
In the presence of macular hemorrhages or edema of the optic disc, narrowing of the visual field, scotomas and light phenomena (flashes or flying flies), eye pain, headache and severe visual impairment appear.
Diagnosis
Since it does not cause obvious symptoms, it is not at all easy to identify this pathological condition, especially in the initial phase. The severity of retinal lesions is related to the general picture (ie the duration and severity of systemic arterial hypertension).
The diagnosis of hypertensive retinopathy is based on anamnesis and on the examination of the ocular fundus, which evaluates the size and course of the blood vessels that supply the retina and ascertains the possible presence of lesions, such as haemorrhages and ischemic areas.
In the initial stages of the disease, this investigation allows to find a generalized or localized arteriolar narrowing, with a reduction in the ratio between the caliber of arterioles and retinal venules. In the later stages, superficial flame haemorrhages and small white foci of retinal ischemia (cottony exudates) are appreciated.
If the retinopathy derives, on the other hand, from a "poorly controlled chronic hypertension, the evaluation can demonstrate the presence of alterations at the level of arteriovenous crossings, diffuse or focal edema and arteriosclerosis with hyperplasia and thickening of the vascular wall. To support these evaluations. retinal fluorangiography (fluorescein angiography) can be performed to highlight early alterations of the retinal vessels and study the evolution of the pathology.
Clinical classification
Based on the alterations of the fundus of the eye, the evolution of hypertensive retinopathy is classified clinically in 4 stages:
- 1st stage: it is characterized by a slight and diffuse arteriolar narrowing at the retinal level.
- 2nd stage: vasoconstriction is accentuated (both diffuse and focal) and the macular arterioles become tortuous; in the vascular tree, some peculiar signs are observed caused by the alteration of the relationship between arterial and venous vessels at the level of their intersections. For example, segmental crushing and narrowing are observed: the vein appears "pinched" or undergoes a sudden displacement after the arteriovenous crossing, due to the compression exerted by the artery that is thrown on it. In other cases, a blood engorgement is created which makes the oat thicker and more tortuous before crossing, while it is thinner and rectilinear once this point is passed. Sometimes, however, a "total vascular occlusion" occurs.
- 3rd stage: alterations are no longer observed only at the level of the vessels; in the back of the eye, in fact, flame haemorrhages appear, diffuse retinal edema and "cotton flock" exudates (ie whitish patches, with faded margins, which correspond to non-perfused areas or areas subject to micro-infarcts). In this phase of hypertensive retinopathy, it is also possible to find "hard" and yellowish exudates, due to the deposition of lipoprotein substances, originating from the extravasations of the retinal vessels, with clear margins and various forms. When edema and exudates affect the macula we speak of "macular star", a condition associated with severe visual impairment.
- 4th stage: swelling of the optic nerve head develops (papilledema due to stasis) and exudative detachment of the retina is possible. In this phase, changes in the color and ophthalmoscopic reflexes of the arteries are found for sclerosis of the vessel wall. The vessels affected by modest alterations appear with a "copper wire" reflection and have a reduced caliber; on the other hand, when hyperplasia and thickening of the vascular walls occur, the hue becomes silver (the sclerotic modifications of the retinal arteries make the light reflection broad and opaque). The fourth stage of hypertensive retinopathy is typically associated with uremia or malignant hypertension.
Treatment
Hypertensive retinopathy is mainly managed through the control of hypertension, an approach that normally prevents the progression of lesions. Drug therapy therefore coincides with that established for increasing systemic blood pressure.
In the event of severe visual impairment, intravitreal injection of corticosteroids or vascular endothelial growth factor (VEGF) antagonists may be useful. In the more advanced stages of hypertensive retinopathy, photocoagulative laser treatment may be indicated to destroy ischemic retinal areas.In this situation, however, visual recovery is difficult.
Who is hypertensive, should regularly undergo a periodic check of the ocular fundus by the ophthalmologist; this examination can provide, in fact, an "information on" the evolution of the hypertensive state at the retinal level and allows to verify the degree of effectiveness of the therapy.