Generality
Rheumatic fever is a generalized inflammatory process, which affects various anatomical areas of the body; the most affected sites are the large joints, the heart, the skin and the nervous system. The disorder has a "curious origin: due to a" bacterial infection, sustained by group A streptococcus, the immune system begins to function incorrectly and to act against the organism to be defended.

Figure: Rheumatic fever affects children the most and arises after streptococcal pharyngitis. From the site: www.stuff.co.nz
From this, various symptoms arise, including joint pain and swelling, heart problems, fever, etc.
To avoid complications, it is important that diagnosis and treatment are timely. Treatment consists of relieving symptoms and preventing the onset of other infections.
What is rheumatic fever?
Rheumatic fever is a generalized inflammatory disease, which is a posthumous complication of group A streptococcal infections. The main sites affected by the inflammatory process are the large joints, heart, skin and central nervous system.
Healing can occur even without treatment, however, in this case, there is a high risk that the disease will leave permanent damage to the patient.
STRETCH OF GROUP A
The bacterium involved in the onset of rheumatic fever is group A streptococcus (Streptococcus Pyogenes), which causes pharyngitis (sore throat) or scarlet fever.
Rheumatic fever can therefore be considered a complication of these infectious diseases.
EPIDEMIOLOGY
In industrialized countries, rheumatic fever is very rare: in fact, it is one person for every 100,000 inhabitants. On the contrary, it is much more common in overcrowded and sanitation-deficient countries, such as some regions of Africa, the Middle East and South America.
Around the world, there are just under half a million cases of rheumatic fever annually.
The most affected individuals are young people (males and females equally), aged between 5 and 15 years. In adults, however, this inflammatory disease is very rare.
Causes
At one time, it was believed that rheumatic fever was caused exclusively by streptococcus group A of pharyngitis or scarlet fever.
Today, however, it is quite convinced that the pathological mechanism is another, more complex and with more protagonists. It seems, in fact, that the inflammation is caused by a malfunction of the immune system, activated to defend the organism from streptococcal bacterial infection.
A FEW MORE DETAILS ™
The immune system, once activated against the bacterium in question, exchanges some physiological molecules of the human body (they seem to be proteins) for molecules of bacterial origin, attacking and destroying them. This triggers the inflammatory process in all those tissues containing this molecule recognized as foreign and dangerous.
It remains to be explained why the immune system, at some point, goes "haywire"; in this regard, some possible risk factors have been identified, but further scientific investigations are needed.
RISK FACTORS
Known risk factors, with a role in immune system malfunction, are:
- Environmental factors. Living in an overcrowded and hygienic-sanitary environment exposes each individual to repeated bacterial infections from group A streptococcus; this means that the probability of getting rheumatic fever is higher than in countries where health measures are at the forefront. This theory is supported by statistical data.
- Genetic factors. Some people are naturally predisposed to developing rheumatic fever, as this predisposition is "written" in their genes. With respect to the environmental component, the theory of genetic factors presents several question marks.
Symptoms and Complications
For further information: Rheumatic Fever Symptoms
The symptoms and signs that characterize rheumatic fever are numerous.
heart, large joints, skin and central nervous system; moreover, rheumatic fever can cause a series of manifestations similar in some respects to those of the flu, such as fever and sore throat. In any case, it is good to remember that each patient represents a case in itself, with a symptomatology that can sometimes be different from the most common one.
A list of the main symptoms is as follows:
- Arthritis of the large joints (knees, hips, wrists and ankles)
- Heart problems, due to inflammation of the myocardium (the muscle of the heart)
- Skin rash
- Sydenham's chorea (it is a particular inflammation of the nervous system)
- Chest pain
- Medium-high fever
- Abdominal pain
- Subcutaneous nodules
- Enlarged lymph nodes in the throat
THE ARTHRITIS
Arthritis is probably the most common symptom of rheumatic fever: in fact, joint pain and swelling affect three out of four people.

Figure: rheumatic fever causes pain and swelling in the large joints of the human body. From the site: www.dinf.ne.jp
The joints involved are usually those of the knees, hips, wrists and ankles, which are painful on both sides of the body.
The onset of this disorder is quite rapid, so much so that in some individuals, arthritis can occur even after just one week after bacterial infection.
HEART PROBLEMS
Heart problems, due to inflammation of the myocardium (the heart muscle), are perhaps the most important symptom of rheumatic fever. This importance is not so much due to the percentage of patients affected (about 30-60%), but rather , to the serious complications that could arise.
An inflamed myocardium impairs the contraction of the heart and, with it, the blood circulation. All this manifests itself with shortness of breath (both after exertion and at rest), persistent sense of fatigue, chest pain and tachycardia.
If not treated properly, cardiac inflammation can cause permanent damage to the anatomical structures of the heart (see complications).
SYDENHAM KOREA
Sydenham's chorea is an inflammatory condition affecting the nervous system. It mainly manifests itself with involuntary jerking movements and uncontrollable body contortions; secondly, it can result in lack of balance, inability to coordinate hand movements and sudden mood swings.
Sydenham's chorea appears almost exclusively in young patients (one case out of four) and, once rheumatic fever is exhausted, it leaves no permanent brain damage.

Figure: the skin rash. The redness usually begins from the neck and then spreads over the entire trunk. From the site: www.iahealth.net
SKIN RASH
The skin rash, or rash, that accompanies rheumatic fever is also called marginal epithelium. It is a painless, non-itchy redness of the skin (ie it does not itch) and characterized by a jagged edge.
It is rare, as it affects one in every 10 young patients, and tends to fade and reappear spontaneously.
WHEN TO SEE THE DOCTOR?
The signs to watch for, because they could indicate that rheumatic fever is ongoing, are:
- A severe inflammation of the throat (pharyngitis), without the classic cold symptoms
- Enlarged lymph nodes in the neck
- Appearance of skin rash, first between the head and neck, then in the trunk
- Difficulty swallowing, due to pharyngitis
- Tongue of intense red color and with small growths
- Fever between 38 ° C and 38.5 ° C
COMPLICATIONS
If not treated properly, rheumatic fever can cause permanent damage to the heart, particularly by affecting the heart valves. Heart valves regulate the flow of blood into and out of the heart and, clearly, their malfunction can impair blood circulation.
Most common heart disease caused by rheumatic fever:
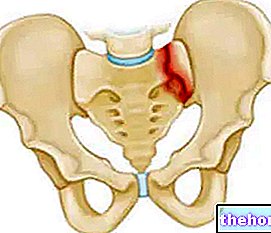
- Valve stenosis
- Aortic insufficiency or mitral insufficiency
- Damaged and weaker myocardium
- Atrial fibrillation
- Heart failure

Figure: the heart and its main anatomical structures. Cardiac complications often involve the valves, above all the mitral and aortic ones.
THE RELAPSES
Those who have already suffered from rheumatic fever are prone to relapses, especially if they become infected with the bacterium again Streptococcus Pyogenes.
Diagnosis
To establish the diagnosis of rheumatic fever, a physical examination of the patient, a thorough blood test, and finally instrumental tests are needed.
OBJECTIVE EXAMINATION
During the physical examination, doctors ask the patient how their symptoms have arisen and how long they have been experiencing them. For example, knowing if an individual has spent a long time in a country where rheumatic fever is easier to get, can be a lot. important.
Then, first-hand assess the condition of the large joints, the presence of fever and signs of Sydenham's chorea, the heart rate and the appearance of the throat.
BLOOD ANALYSIS
The blood of a patient with rheumatic fever has particular characteristics, which can be highlighted with certain tests.
So-called erythrocyte sedimentation and C-reactive protein (CRP) tests show whether there is ongoing (high values) or not (normal values) an "inflammation" within the body.
The antistreptolysin title, on the other hand, is a test that aims to search for the presence of anti-streptococcal antibodies. If these are indeed present, it means that there has "been a" bacterial infection in the recent past.
INSTRUMENTAL DIAGNOSTICS
The instrumental examinations consist of the electrocardiogram (ECG) and the echocardiogram.
The ECG measures the electrical activity of the heart, showing whether or not there are changes in the beat.
The "echocardiogram, on the other hand, is an" ultrasound, which provides detailed images of the main anatomical structures of the heart (valves, atria and ventricles).
In both cases, these are harmless tests for the patient, which the doctor advises to repeat periodically, because heart problems from rheumatic fever do not appear immediately.
JONES CRITERIA
Below is a table with the so-called Jones criteria, useful for the doctor to determine whether or not it is rheumatic fever. The criteria are divided into major and minor: we speak of rheumatic fever when the patient has at least two major criteria or two minor criteria and at least one major.
The major criteria
- Obvious cardiac anomalies (chest pain, arrhythmia, shortness of breath, etc.)
- Severe pain and joint swelling
- Involuntary body movements (Sydenham's chorea)
- Non-itchy, painless skin rash
- Subcutaneous nodules
The main minor criteria
- Medium-high fever
- Blood tests for "ongoing inflammation."
- Slight pain in the joints
- Mild arrhythmia
Treatment
There is no specific cure for rheumatic fever; we must wait for this to heal spontaneously. However, there are therapeutic countermeasures that have the following objectives:
- Relieve symptoms and reduce the risk of permanent damage
- Completely eliminate streptococcus from the body
- Protect from future bacterial infections
THE ANTI-INFLAMMATORS
Anti-inflammatories are administered to the patient to relieve and moderate the symptoms of rheumatic fever: above all, pain and swelling in the large joints and inflammation of the myocardium.
The drugs most frequently used are: NSAIDs (ibuprofen or naproxen), aspirin and, in severe cases, prednisolone.
Aspirin and prednisolone require special attention during their intake, as they can trigger serious side effects. The first, in young patients, can cause Reye's syndrome; the second is a corticosteroid, a powerful anti-inflammatory capable of promoting osteoporosis. hypertension, weight gain, etc.
THE ANTIBIOTICS
Antibiotics (penicillin and derivatives) are taken by the patient to completely eliminate the streptococcus and to protect it from future bacterial infections (prophylaxis), which could cause the rheumatic fever to return.
The best way to prevent a relapse is to have intravenous injections of the antibiotic every two to three weeks, for several years.
THE ANTICONVULSIVANTS
Anticonvulsants, such as valproic acid, are given to patients who show the typical signs of Sydenham's chorea.
For further information: Medicines for the Treatment of Rheumatic Fever "
THE REST
The doctor advises to remain at rest so as not to tire the patient and to shorten the healing time. It is particularly indicated if the individual with rheumatic fever suffers from severe heart problems.
Refraining from physical activity allows for easier resolution of myocardial inflammation.
Prognosis and prevention
The prognosis for rheumatic fever largely depends on when treatment is started.
If both diagnosis and treatment are timely, recovery is quick and, with a good chance, uncomplicated.
Conversely, a late diagnosis and therapy affect the recovery process, as there is a greater risk of complications and the patient being subject to relapses.
PREVENTION
To prevent the onset of rheumatic fever, it is very important to scrupulously treat group A streptococcal infections. With the appropriate therapies, the risk of worsening the situation is minimal, especially in countries with state-of-the-art health measures.
As for those who have already contracted rheumatic fever, the best recommendation is to undergo periodic checks and prophylaxis.