Furthermore, it allows to evaluate the functioning of a pacemaker or an implantable cardioverter defibrillator, in all those subjects who are wearers of devices for the normalization of the heart rhythm.
There are three types of electrocardiogram: the resting ECG, the dynamic ECG according to Holter and the stress ECG.
Cardiologists are able to understand the state of health of the heart and its functioning from the aspect of the electrocardiographic trace.
, that is, a doctor who specializes in cardiology.
Heart: Anatomy and Function in Brief
The heart is an unequal organ, which can be divided into four cavities (the right atrium, the left atrium, the right ventricle and the left ventricle) and is made up of a very particular muscle tissue: the myocardium.
The peculiarity of the myocardium lies in the ability to generate and conduct the nerve impulses by itself for the contraction of the atria and ventricles.
The source of these impulses, which are comparable to electrical signals, resides in the right atrium and is called the sinoatrial node.
The sino-atrial node has the task of marking the correct rate of contraction of the heart organ (the so-called heart rate), in order to guarantee a normal heart rhythm.
Normal heart rhythm is also called sinus rhythm.
to detect:
- The presence of cardiac arrhythmias.
A "cardiac arrhythmia is" an alteration of the normal heart rhythm (sinus rhythm).
The normal heart rhythm of an adult human has a resting contraction rate between 60 and 100 beats per minute. - A "ischemia or myocardial infarction, possibly secondary to a narrowing or complete occlusion of the coronary arteries of the heart (N.B: myocardial infarction and heart attack are synonymous).
The coronary arteries of the heart are the arterial vessels that supply the myocardium with oxygenated blood and nutrients.
In medicine, the narrowing and complete occlusion of the coronary arteries of the heart takes the generic name of coronary artery disease or coronary artery disease. - The presence of structural changes in the heart cavities, atria and / or ventricles.
The structural alterations of the heart cavities include conditions such as: dilated cardiomyopathy, hypertrophic cardiomyopathy, left ventricular hypertrophy and enlarged heart.
Under such circumstances, the walls of the atria and / or ventricles may thicken or stretch. - The outcomes of a previous heart attack.
The heart attack leaves indelible marks both anatomically and functionally.
Patients who have suffered a myocardial infarction should periodically undergo an electrocardiogram to monitor the condition of their heart. - The presence of cardiac conditions, characterized by an "alteration of electrical conduction. Some examples of these cardiac conditions are: long QT syndrome and bundle branch blocks (right or left).
In addition, the electrocardiogram allows you to evaluate:
- The operation of pacemakers and similar devices (such as the implantable cardioverter defibrillator), in subjects who clearly carry them.
- The effects on the heart of those drugs that could, in some circumstances, alter the frequency or electrical conduction of the heart.
In number of 12 or 15, the electrodes for an ECG at rest are in fact metal plates, applicable to the skin in various ways: through an adhesive portion (in this case they resemble patches), through suction cups or through an adhesive gel.
After applying the electrodes to the patient, the "usual" medical assistant or cardiologist starts the electrocardiograph and the recording begins.
The recording phase usually lasts a few seconds, which is long enough to obtain a trace sufficient for an evaluation of heart function.
During the actual procedure, the patient must breathe regularly - unless otherwise indicated - but must not move or speak, as doing so could distort the outcome of the examination.
The duration of an electrocardiogram at rest, from when the patient enters the doctor's office until the recording ends, is a few minutes.
Curiosity: if the patient under examination is a man with a particularly rich chest, the medical assistant shaves the aforementioned anatomical area, to avoid the risk of premature detachment of the electrodes.
Dynamic Electrocardiogram According to Holter

Figure: electrodes of a typical resting EKG instrument. The reader may notice how these metal plates have the outward appearance of patches.
The Holter electrocardiogram is a type of electrocardiogram which, thanks to the use of a portable electrocardiograph, allows the monitoring of cardiac function over a certain period of time, generally 24-48 hours.
The idea of creating a portable electrocardiograph, which would record cardiac function for a certain number of consecutive hours, arose from the need to "capture" those discontinuous arrhythmias, with sporadic appearing, that a resting ECG struggles to highlight.
Generally the task of a physician's assistant, the installation of the portable electrocardiograph is a simple, quick and painless procedure, which involves the application of the recording electrodes (only) on the chest. The electrodes for a Holter electrocardiogram are metal plates with a adhesive portion.
From a strictly procedural point of view, the Holter electrocardiogram can be divided into two consecutive phases:
- The phase of recording the rhythm and electrical activity of the heart. It is the first of the two phases and goes from when the medical assistant installs and operates the portable electrocardiograph to when the assistant or a colleague removes it.
In this phase, the instrument records and saves the patient's cardiac function in an internal memory. - The graphic translation phase of what was recorded in the previous phase. It is, in fact, the phase dedicated to the creation of the track with its characteristic waves.
It is up to the "usual" medical assistant or a cardiologist, who extrapolate the data from the portable electrocardiograph through a specific computerized device.
The interpretation of the resulting trace is obviously up to the cardiologist.
During the registration phase, the patient can continue to carry out their normal daily activities, clearly taking care not to bump the device and not to detach the electrodes.
Curiosity: in some very special cases, the dynamic electrocardiogram according to Holter can last even 7 (seven) days.

Electrocardiogram Under Stress
The electrocardiogram under stress involves recording the heart function of an individual, while the latter is performing physical exercise of a certain intensity or - but more rarely - after taking a drug that acts on the heart and causes the same effects of physical exercise.
The purpose of the electrocardiogram under stress is to see the behavior of the heart during physical exertion: how the heart rhythm varies, which heart problems can cause the body to demand more blood, etc.
As in the previous two cases, the installation of the electrodes - which usually have the appearance of adhesive plasters - is the responsibility of a medical assistant.
The area of application of the recording elements is only the thorax, as the involvement of other anatomical areas would prevent the patient from moving easily during physical exercise.
The classic physical exercises foreseen during an electrocardiogram under stress are: walking on a Tapis Roulant or ride on one exercise bike.
The duration of an exercise electrocardiogram, from when the patient enters the doctor's office until the recording ends, is a few tens of minutes.
It should be noted that the possible onset of a cardiac complication during an exercise electrocardiogram is due to physical exercise and not to the electrocardiograph.
, which can arise as a result of an "impaired conduction of the nerve impulse through the myocardium or as a result of heart disease such as a myocardial infarction or cardiomyopathy."
In the next subchapters, readers will be able to appreciate the electrocardiographs of some of the most well-known heart conditions.
Clearly, in order to understand the particularities of these traces, it is also necessary to report the result of an electrocardiogram performed on a person who is healthy from a cardiological point of view.
Normal Electrocardiogram (Normal ECG)
As can be seen from the figure below, the electrocardiographic trace of a healthy person has 5 characteristic waves, identified with the capital letters P, Q, R, S and T.
- Wave P: represents the contraction of the atria of the heart. In technical jargon, doctors define it as the "depolarization wave of the atria."
The P wave lasts on average 0.08 seconds (but can range from 0.05 seconds to 0.12); if it lasts 0.08 seconds, it means it covers 2 small squares on the graph paper sheet.
Immediately after the "wave P, c" is a straight section that ends in correspondence with the waves Q, R and S and which takes the name of interval PR. The PR interval expresses the time it takes for the depolarization wave to propagate from the sinoatrial node along part of the electrical conduction system of the heart, present on the myocardium (specifically, the atrioventricular node and bundle of His).
The PR interval has a duration that varies between 0.16 seconds and 0.2 seconds, so it covers 4 to 5 small squares. - Q, R and S waves: together, these waves form the so-called QRS complex. The QRS complex represents the contraction of the ventricles and, in technical jargon, takes the name of the ventricle depolarization complex.
Typically, the QRS complex lasts 0.12 seconds, so it covers about 3 squares.
During the contraction of the ventricles, relaxation of the atria, which previously contracted, takes place. In medical parlance, such relaxation is known as repolarization of the atria or return to rest of the atria. - T wave: expresses the relaxation of the ventricles. In medical jargon, this relaxation is called repolarization of the ventricles or return to rest of the ventricles.
After the "T wave, c" is a second horizontal section, which ends at a subsequent P wave. The next P wave represents the beginning of a new cycle of depolarization and repolarization of the atria and ventricles.
Taken together, the P, Q, R, S and T waves make up the so-called PQRST complex.
Cardiologists refer to the interval between two PQRST complexes as the "R-R interval." The R-R interval corresponds to one cardiac cycle.
The choice of entrusting the R waves of two consecutive PQRST complexes with the task of identifying the beginning and end of a cardiac cycle is due to the fact that, as can be seen from the trace below, the R wave is particularly evident.

- PR interval: 0.16 - 0.20 seconds
- ST interval: 0.27 - 0.33 seconds
- QT interval: 0.35 - 0.42 seconds
- QRS interval: 0.08 - 0.11 seconds
Curiosity: electrocardiogram of a deceased person
The trace resulting from an electrocardiogram given to a deceased, whose heart has stopped beating, appears as a straight line, devoid of any waves

Atrial Fibrillation Echocardiogram
Atrial fibrillation is an "arrhythmia that makes the heart beat very fast and irregular. It can have the characteristics of a sporadic phenomenon or a chronic phenomenon. If it is sporadic, it is generally also very intense; if it is chronic, it is usually of reduced intensity.
Atrial fibrillation is caused by an abnormal generation of impulses that contract the atria of the heart. This anomalous generation, in fact, causes the walls of the atrial cavities to undergo continuous and incessant stresses.
During atrial fibrillation, the atria have a contraction rate of approximately 350-400 beats per minute. This increased contractile frequency of the atria has repercussions on the ventricles, also strongly altering their frequency of contraction.
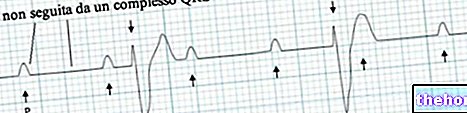
The electrocardiogram of a person with atrial fibrillation has the following characteristics:
- Absence of P waves. This denotes the contraction defect of the atria, typical of atrial fibrillation.
- Irregular straight sections.
- QRS complexes of irregular shape.

Atrial Flutter Echocardiogram
Atrial flutter is an "atrium-based" heart rhythm disorder, like atrial fibrillation.
Its onset coincides with a very rapid, irregular heartbeat of varying intensity.
Compared to atrial fibrillation, the rate of contraction of the atria is slightly lower: in an atrial flutter, in fact, the atria contract with a rate of approximately 240-300 beats per minute.
This high rate of contraction of the atria can have repercussions on the contractile rate of the ventricles: when it occurs, cardiologists speak of paroxysmal atrial flutter; when it does not, they speak of permanent atrial flutter.
The electrocardiogram of a person with atrial flutter has the following important feature:
- Presence of a minimum of 2 to a maximum of over 10 P waves before each QRS complex.
This succession of different P waves is called a "sawtooth" path.
The large number of P waves indicates a disturbance of the atria.

Echocardiogram Myocardial Infarction
Myocardial infarction, or heart attack, is the pathological process by which the flow of blood destined for the myocardium is inadequate to the demands, causing the death of a more or less extended area of the heart muscle.
Often caused by atherosclerosis, this serious condition coincides with the necrosis (ie death) of the myocardial tissue, resulting in a reduction in the contractile capacity of the heart.
The most classic symptoms of heart attack include: dyspnoea, chest pain, heartbeat, cyanosis, hypoxia, nausea, vomiting, confusion and various kinds of alterations in the heart rhythm.
There are various types of myocardial infarction. The main types are: lower myocardial infarction, anterior myocardial infarction, anterolateral myocardial infarction and posterior myocardial infarction.
Each type of heart attack determines, on the electrocardiographic trace, similar anomalies but with different localization.
Among these anomalies, the most characteristic are:
- Presence of very deep Q waves, with disappearance of the respective successive R waves.
- Disappearance of the S wave, which merges with the T wave. The result is a more or less rounded convexity, which cardiologists call ST segment or ST segment elevation.

Ventricular Fibrillation Echocardiogram
Ventricular fibrillation is an "arrhythmia that affects the ventricles and alters the characteristics of the heartbeat in a profound way.
In fact, the latter takes on a decidedly increased frequency and speed, becomes irregular, loses coordination, constantly changes its intensity and, finally, is ineffective from a mechanical point of view.
The presence of ventricular fibrillation affects cardiac output. Changes in cardiac output strongly expose the patient to episodes of cardiac arrest or sudden death.
The electrocardiogram of a person with ventricular fibrillation has the following characteristics:
- Waves with irregular, bizarre and random shapes ("box of worms")
- QRS complexes and / or P waves that are difficult to identify.
- Deviations of straight sections.

ECG Complete Atrioventricular Block
Complete atrioventricular block consists of an interruption, which takes place between the atrium and the ventricle, of the electrical signals that contract the heart. This leads to a lack of synchrony between the various cardiac cavities.
The electrocardiogram of a person with complete atrioventricular block has the following characteristics:
- Absence of relationship between P waves and subsequent QRS complexes.
- Altered QRS complexes, due to abnormal ventricular conduction.
- The ventricles depolarize independently of the atria.
ECG Sinus Tachycardia
Sinus tachycardia is an "arrhythmia characterized by" an increase in the rate and speed of the normal heart rhythm (or sinus rhythm). It does not involve any irregular heartbeat and is perhaps, among the existing arrhythmias, the most widespread.
Usually, it is the consequence of events, such as strenuous exercise, a strong emotion or a simple fever, after which the heart rhythm returns to normal.
Much more rarely, it is the result of severe heart disease or anemia.
The electrocardiogram of a person with sinus tachycardia has the following characteristics:
- P waves with a frequency greater than 100 beats per minute. Remember that the normal heart rhythm is between 60 and 100 beats per minute.
- R-R interval much shorter than normal, in terms of squares on graph paper.
- Faster but steady pace.

ECG Sinus Bradycardia
Sinus bradycardia is a reduction in normal heart rate (sinus rhythm), without any irregular heartbeat.
Various conditions / circumstances can establish a state of sinus bradycardia, including: night sleep, good physical shape, hypothermia, hypothyroidism, digitalis, beta-blockers, calcium channel blockers or quinidine, diphtheria, rheumatic fever, etc.
The electrocardiogram of a person with sinus bradycardia has the following characteristics:
- P waves with a frequency lower than 60 beats per minute (N.B: in the combined graph the frequency of the P waves is equal to 45 beats per minute).
- Slower but steady pace.
- R-R interval much longer than normal, in terms of squares on graph paper.

ECG Long QT Syndrome
Long QT syndrome is a rare heart condition, which involves lengthening the repolarization times of the ventricles. In other words, long QT sufferers have a heart whose ventricles take longer than normal to relax and prepare for "another contraction."
This delay in the repolarization of the ventricles favors the onset of syncope, convulsions and severe cardiac arrhythmias, such as ventricular fibrillation.
The long QT syndrome owes its particular name to the characteristic electrocardiogram presented by carriers: in the electrocardiographic trace of these subjects, the QT interval lasts for more than 0.42 seconds, which represents the maximum threshold of normality.

ECG in a patient with a ventricular pacemaker
A pacemaker is a small electronic device, capable of normalizing, through the release of electrical impulses, the heart contractions of people with a heart that is too slow, too fast and irregular.
Implanted just below the collarbone, a generic pacemaker includes these components: a pulse generator, enclosed within a metal container, and one or more cables called leads.
The leads represent the elements for conducting electrical impulses, produced in the generator, to the heart.
Based on the number and location of leads, a pacemaker can be: single-chamber, dual-chamber and biventricular.
The electrocardiogram of a person with a single chamber ventricular pacemaker has the following characteristics:
- Absence of the P wave, because the center of generation of electrical impulses changes (it is no longer the sinoatrial node but the pacemaker).
- Presence of a small tip (spike) near the QRS complex.
- Wider QRS complexes, compared to the QRS complexes of a normal ECG.


-cos-come-si-svolge.jpg)