Many of the pathogens that enter the respiratory tract pass through the adenoids, which therefore have a predominantly defensive function.
Sometimes, especially in children, the adenoids can be affected by occasional or recurrent infections, which in some cases make it difficult to breathe through the nose. The most common pathologies affecting the adenoids can make them hypertrophic (enlarged adenoids) or inflamed (adenoiditis).
coming from outside. White blood cells circulate through the adenoids and other lymphoid tissues, reacting to potential pathogens that enter the body. Histologically, adenoids, unlike other types of tonsils, have a ciliated columnar pseudostratified epithelium.

Function
Adenoids perform immune functions: they help the body defend the organism from infections by trapping and eliminating bacteria and viruses that invade the tissues around the orifices of the nasal and oral cavities.
DEVELOPMENT and INVOLUTION
Adenoids are lymphatic formations present from birth, which develop progressively reaching their maximum size at the age of approximately 3-5 years. Normally, in children, a soft mound forms in the upper and posterior part of the nasopharynx, just above and behind the uvula. At the age of about 7, the adenoids undergo an involutionary process, reducing their size due to the physiological atrophy of the adenoid tissue, which makes them barely visible during adolescence. In adulthood, they become virtually inactive.
Although they are useful in preventing infections during early childhood, the body has more effective means of fighting bacteria and viruses. For this reason, if they grow excessively and cause significant breathing difficulties, they are often surgically removed along with the palatine tonsils.
: inflammation of the adenoids, often caused by bacterial or viral infections. Infectious processes affecting the adenoids can cause other health problems, including sinusitis and serious respiratory disorders, especially during night rest.Signs and symptoms. Acute adenoiditis is characterized by fever, nasal respiratory obstruction, snoring, obstructive sleep apnea and rhinorrhea with serous secretion (in viral forms) homuco-purulent (in bacterial forms). This typical presentation of adenoiditis makes it difficult to distinguish from to a common cold.
Symptoms due to a "viral infection of the adenoids usually regress spontaneously after 48 hours, while bacterial adenoiditis can persist for up to a week.
Infections of the adenoids can cause a number of complications due to the extension of the inflammatory process to nearby tissues and organs, including:
- Middle ear infections (otitis): the adenoids are located near the Eustachian tube, channels that connect the nasopharynx with the middle ear. Infections can spread from the nasopharynx to the ears and cause serous or purulent otitis, also affecting hearing.
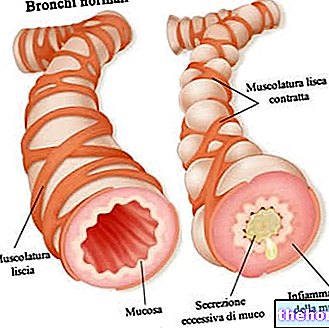
- Sinusitis and respiratory tract infections: Bacteria or viruses can infect other sites, such as the bronchi (bronchitis) or lungs (pneumonia).
Responsible pathological microorganisms
Viruses that can cause adenoiditis include Adenovirus, Rhinovirus, and Paramyxovirus. The bacteria mainly involved are: Streptococcus pyogenes, Streptococcus pneumoniae, Moraxella catarrhalis And Staphylococcus aureus.
Diagnosis
The condition is diagnosed based on the medical history and physical examination. Adenoids cannot be visualized easily, so doctors can locate the inflammatory process using a fiber-optic endoscope. Endoscopy can confirm the diagnosis by directly highlighting the inflamed adenoids. A microbiological culture and blood test can help find the cause of the symptoms by identifying the organism involved. Occasionally, x-rays or other imaging techniques may be done to check the size of the adenoids.
Pharmacological therapy
In the case of viral adenoiditis, the administration of analgesics and antipyretics is often sufficient. Bacterial forms, on the other hand, can be treated with antibiotics, such as amoxicillin-clavulanic acid or a cephalosporin.
Surgical treatment
If symptoms are severe or persistent, it is possible to surgically remove the adenoids, using an adenoidectomy. Often, this option becomes necessary when the adenoiditis does not respond to drug therapies and tends to become chronic. Surgical removal is appropriate even when adenoids impede normal breathing. After surgery, many individuals with recurrent adenoiditis report significant improvement.
and difficulty swallowing;The airway obstruction can reduce the flow of air from the nose, causing the person to breathe through the mouth.
In addition to hindering breathing, adenoids can block the Eustachian tubes; these ducts connect the middle ear to the back of the nose, help the outflow of liquids that accumulate in the middle ear and maintain the right air pressure inside the ear. The clogging of this drainage system it can lead to recurring infections and impaired hearing. If a child cannot hear sounds clearly, it can have consequences on learning, development and social interaction, so it is important that an "ear infection" is diagnosed and treated properly.
For further information: Hypertrophic Adenoid Symptoms;
Adenoidectomy may be necessary if the adenoids become hypertrophic due to:
- Infection with bacteria or viruses: although the infection can resolve itself, the adenoids can remain excessive in size;
- Allergies: allergens (substances that trigger an allergic reaction) can irritate the adenoids and cause them to swell;
- Congenital: the fetus can develop adenoids in the womb; at birth they may be enlarged.
Other indications for adenoidectomy include:
- Enlargement of the adenoids interferes with breathing, especially at night.
- Recurrent or persistent otitis media in children aged 3-4 years and older (may interfere with language development);
- Relapsing and / or chronic sinusitis.
After surgery, most patients:
- Has fewer throat infections, which occur in a milder form;
- Has fewer ear infections;
- Breathe better through the nose.
How is an "adenoidectomy performed
Before the operation. The mouth and throat tend to bleed more easily than other areas of the body, so the doctor may request a pre-operative blood test. In the week preceding the surgery, no medicines should be given that they could affect blood clotting, such as "ibuprofen or" aspirin.
Adenoidectomy involves the administration of a general (less commonly local) anesthetic and is performed in about 30 minutes. In most cases, the patient can go home the same day of the surgery.
How are adenoids removed? The operation is performed through the mouth and involves removal of the adenoids by currettage (scraping) or ablation. To seal the wound, the surgeon may cauterize or apply absorbable sutures.
Adenotonsillectomy. If the patient is prone to severe or frequent attacks of tonsillitis (tonsil infection), simultaneous surgical removal of tonsils and adenoids may be indicated. This procedure is called adenotonsillectomy.
Trans-tympanic drainage. In case of otitis media, adenoidectomy can be completed with a tympanostomy: through a small cut in the eardrum, a small ventilation tube is placed in the ear to drain serous, mucous or purulent secretions. The trans-tympanic drainage helps to drain the fluid that accumulates in the middle ear during the inflammatory process and reduces the infection.
Recovery from an "adenoidectomy
Following an adenoidectomy, the patient will need rest for several days. Full recovery usually takes 1-2 weeks. Some medications are prescribed to reduce pain and swelling. The patient will normally be able to start drinking fluids. 2-3 hours after the operation.
Possible postoperative complications
Adenoidectomy is a low-risk procedure that rarely causes complications. It is relatively common, quick and easy to do. However, as with all surgeries, there is a small risk that complications such as bleeding, allergic reactions to anesthesia or infections may occur.
Following an adenoidectomy, some patients may experience some minor health problems, such as a sore throat, difficulty swallowing, earache, stuffy nose, halitosis (bad breath) and a change of voice. However, most of these disorders are temporary, rarely require specific treatment, and tend to resolve within one to two weeks (they should not last longer than four weeks).
Although adenoidectomy effectively reduces the incidence and severity of infections, it must be considered that adenoids represent one of the first barriers to microbial invasions and, if removed, can facilitate the penetration of these germs into the body.