Generality
Cholesteatoma is a middle ear disease characterized by an unusual collection of epithelial cells near the eardrum or the three ossicles.

Figure: A live cholesteatoma. From the site: www.ao.pr.it
The accumulation of this mass of cellular debris is very often due to bacterial infections of the ear canal, but not only.
The main symptom of cholesteatoma is hearing loss (hypoacusis): at the beginning, it is moderate; subsequently, when the formation expands, it becomes much more intense. Early diagnosis is essential to prevent the patient from experiencing complications, even unpleasant ones; the pressure exerted by the cholesteatoma could in fact damage the surrounding structures.
Surgery is used to remove cholesteatoma. Despite the invasiveness of the operation, the resulting benefits recommend that you undergo the operation.
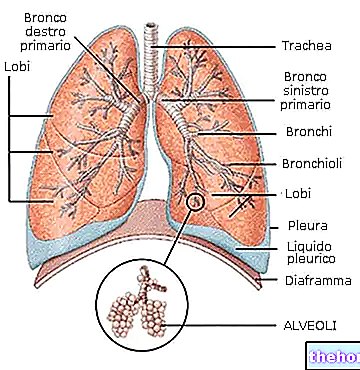
Anatomy of the ear
The ear is divided into three parts:
- External ear
- Middle ear
- Inner ear
The outer ear starts from the auricle and ends where the eardrum is located.
The middle ear is located behind the eardrum and has three small bones: the hammer, the anvil and the stirrup. It communicates with the nose, through a duct called the Eustachian tube. Therefore, air passes inside the middle ear.
The inner ear is the area in which the cochlea and semicircular canals are located. The cochlea is the organ of hearing; the semicircular canals, on the other hand, constitute the organ of balance.
THE THREE BONES OF THE MIDDLE EAR
The three ossicles, hammer, anvil and stirrup, are so called due to their resemblance to the three tools used by the blacksmith during his craftsmanship.
The hammer is the small bone placed in contact with the eardrum. The stirrup connects with the cochlea. The anvil, finally, connects the hammer and the stirrup and is interposed between them.
SOUND WAVES AND HEARING
How does the ear and the perception of sounds work?
The sound waves penetrate the external ear and reach the eardrum. Struck by the sounds, the eardrum vibrates. This vibration is transmitted to the three ossicles, which are set in motion. The hammer begins to move, then the anvil and, finally, the anvil. the bracket. In other words, the movement of one bone determines the movement of the next. It is the so-called ossicular chain.
From the stirrup, the sound signal passes to the cochlea. The latter translates the sound into a nerve signal, which is routed to the brain for final identification.
What is cholesteatoma?
The term cholesteatoma identifies an "unusual collection of squamous epithelial cells, corresponding to a small niche, in the middle ear." This accumulation has the appearance of a pearly-white mass, which progressively increases its volume with time.
The presence of a cholesteatoma poses a threat to the hearing abilities of those afflicted with it, as it can also cause complete deafness.
What are squamous epithelial cells?
When we speak of epithelial cells, or epithelial tissue, we refer to lining cells, present both inside and outside the body. For example, c "is" the epithelium of the skin, mouth, vagina, pulmonary alveoli, etc.
Squamous (or paving) epithelial cells have a flat shape and have a slightly raised nucleus, which resembles a scale. There are different subgroups of squamous epithelial cells: there are "keratinized", "non keratinized", simple, etc .; their appearance depends on the position and the organ they cover.
EVOLUTION OF THE COLESTEATOMA
How does cholesteatoma evolve?
In its initial stages, cholesteatoma affects and damages the eardrum and the three ossicles of the middle ear. Subsequently, it expands, invading the structures of the inner ear (cochlea and semicircular canals) and even the mastoid portion (or mastoid process) of the temporal bone of the skull. The worst forms of cholesteatoma, in fact, penetrate to the brain, causing brain infections with unpleasant consequences.
IS THE COLESTEATOMA A CANCER?
The name cholesteatoma could suggest a malignant tumor pathology, but it should be specified that it has no cancerous origin.
EPIDEMIOLOGY
Cholesteatoma is a rare disorder that affects one in 10,000 people every year. It can arise at any age, with no particular preference.
Some statistical studies report that, among 1,000 people with various hearing problems, only one case has cholesteatoma.
Causes

Figure: A live cholesteatoma. Modified from the site: http://chroniclescamera.blogspot.it/
The exact cause of cholesteatoma has not yet been fully clarified. According to the most accredited hypothesis, the abnormal collection of squamous cells is due to an incorrect cell turnover of the internal epithelial lining of the auditory canal. In other words, in the absence of the disorder, the ear canal replaces its own epithelial cells, creating new ones and eliminating the old ones. In cases of cholesteatoma, however, these cells instead of flaking and dispersing (as "it is usually) accumulate in a point of the middle ear. This is how the pearly-white mass, mentioned above, is created.
ORIGIN OF THE DISORDER: WHY DO THE COLESTEATOMA ARISE?
Two types of cholesteatoma have been distinguished, different in origin:
- Congenital cholesteatoma. Present since birth, it is characterized by the growth of the epithelial mass behind the eardrum.
- Acquired cholesteatoma. Typical of adulthood, it is the consequence of chronic and recurrent ear infections, which close and block the passage of air through the Eustachian tube. This impediment causes the eardrum to be sucked inwards, forming, in this way, a kind of small housing. Here, old squamous epithelial cells accumulate, after replacing them with new ones, and remain trapped in them. It is a time-consuming process, thus explaining why it appears in adulthood.
Acquired cholesteatoma is the most common form of cholesteatoma; in fact, congenital forms are rare.
Symptoms and Complications
Cholesteatoma usually affects only one ear, causing the following symptoms and signs:
- Loss of hearing (hypoacusis)
- Foul-smelling otorrhea
- Tinnitus (so-called "whistles" in the "ear)
- Perforation of the eardrum
- Headache
These manifestations, when cholesteatoma is in its infancy, are mild and do not cause particular disturbance to the patient. Over time, however, the collection of epithelial cells expands, aggravating the entire symptomatology: the three ossicles are involved first and then the structures of the inner ear (cochlea and semicircular canals).
What is otorrhea?
When we talk about otorrhea, we refer to any discharge from the ear canal, due to an "infection of the middle or external ear". Depending on the pathology that originates it, otorrhea can be haematic, purulent, muco-purulent, foul-smelling, watery or mucoid. The possible causes of octopus are: trauma, ear carcinoma, acute otitis and chronic otitis of the middle ear. , cerebrospinal fluid leaks or eczema.
Often, oterrea goes unnoticed, until the causes, which trigger it, worsen further.
HYPOACUSIA
Hearing loss is classified into conductive, sensorineural or mixed (conductive-sensorineural). It is conductive when only the three ossicles are affected (middle ear); sensorineural if only the cochlea and semicircular canals are involved (inner ear); mixed when both are affected. the structures of the middle ear and those of the inner ear.
In cases of cholesteatoma, hearing loss is always of the conductive type. Subsequently, if the collection of squamous cells also affects the cochlea, it can become a mixed type. Another "ear disease", also initially conductive and then mixed, is otosclerosis.
COMPLICATIONS
In light of the above, if cholesteatoma is not treated properly, it can give rise to various complications; the main ones are:
- Damage and possible destruction of the three small bones of the middle ear.
Features: the cholesteatoma, as it grows, also affects the three ossicles.
Aftermath: possible complete and permanent deafness. - Damage to the mastoid portion (or mastoid process) of the temporal bone.
Features: the mastoid bone is connected to the middle ear, via the tympanic cavity, and is composed of numerous cells filled with air. When the cholesteatoma expands, it invades these regions, infecting and destroying them.
Aftermath: brain abscess, meningitis, bone erosion, hearing loss, etc. - Damage to the cochlea and semicircular canals.
Aftermath: permanent deafness, dizziness and loss of balance. - Damage to the facial muscles.
Aftermath: paralysis of the muscles of the face. - Erosion of other bony portions of the skull, located around the ear.
Aftermath: infections, meningitis, brain abscess etc.
Diagnosis
The preliminary diagnosis is based on the detection of the typical symptoms of cholesteatoma: hearing loss, tinnitus and otorrhea. After that, further investigations are needed, such as:
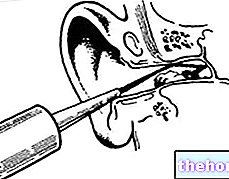
- Otoscopic examination
- Audiometric tests
- Ear swab
- CT scan (computed axial tomography)
WHICH SPECIALIST TO CONTACT?
An individual, who experiences the classic symptoms of cholesteatoma, can refer to both an otolaryngologist and a general practitioner.

Figure: CT scan of a patient with cholesteatoma. From the site: www.infirmus.es
Both, in fact, by means of the otoscope, are able to detect the white-pearly mass of squamous cells, located at the level of the middle ear, and a possible perforation of the eardrum.
The otoscope is an instrument with a small light and a magnifying glass.
AUDIOMETRIC EXAMINATIONS
Audiometric examinations take place in a hospital and, to take care of them, is an audiometrist technician. The purpose of these tests is to define the degree of hearing loss (mild or severe).
The most commonly performed tests are the Rinne test and the Weber test; they are both fast and non-invasive.
Results, in cases of cholesteatoma:
Rinne test
Negative, as long as the hearing loss is conductive (positive results are obtained in cases of sensorineural hearing loss).
Weber test
Higher perception of sounds, in the ear with cholesteatoma.
EAR PAD
As we have seen, one of the typical signs of cholesteatoma is malodorous otorrhea. The bad smell is due to the presence, in the secretion, of a bacterium, Pseudomonas. To identify this germ, responsible for chronic infections in the ear canal, you need an ear swab on which to carry out the appropriate laboratory investigations.
CT (COMPUTERIZED AXIAL TOMOGRAPHY)
This examination, which is slightly invasive because it uses ionizing radiation, shows whether the cholesteatoma has expanded and if it has affected the mastoid process or other areas of the brain.
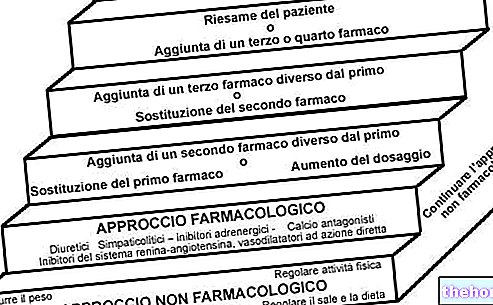
Treatment
Cholesteatoma therapy usually consists of surgical removal of the squamous cell mass. However, this operation is not suitable for all patients; therefore, in these cases, the treating physician is forced to resort to alternative countermeasures, less invasive but also less effective.
THE SURGICAL INTERVENTION
The removal of the choleasteatoma can be carried out, after general anesthesia, through two procedures:
- Tympanoplasty associated with mastoidectomy. This technique involves the incision of the mastoid process (ie the portion of the temporal bone located behind the ear), in order to have free access to the auditory canal. Once the section has been made, the cholesteatoma, contained in the ear, is eliminated. If this has also affected the eardrum and the three ossicles, the latter must be replaced with prostheses. Furthermore, if the infiltration of squamous epithelial cells has reached part of the mastoid bone, the affected areas are removed. hospitalization and lasts several hours.
- The closed technique tympanoplasty. Through this procedure, the ear canal is accessed without removing any bone walls. Many small incisions are made, which allow the cholesteatoma to be removed gradually from the areas where it is wedged. If the eardrum and the three ossicles are damaged, they are repaired or replaced, as in the previous case. The surgery requires hospitalization and lasts several hours.
The first surgical procedure is clearly much more invasive than the second. However, it has more benefits than risks, especially when compared to closed-technique tympanoplasty. In fact, the risk of the cholesteatoma re-forming is very low and complications are very rare events. On the contrary, with the second surgical technique, it is possible that the mass of squamous cells is not completely removed and this can result in a relapse after a short time.
Procedure of intervention
Complications
- Dizziness
- Permanent deafness
- Damage to the facial nerves (paralysis)
NON-SURGICAL TREATMENT
If general anesthesia represents a risk to the patient's health, non-surgical treatment is opted for. The countermeasures, in these cases, consist of a sort of "ear washes", which remove debris and cholesteatoma cells. as invasive as a "surgical operation, these interventions have three disadvantages:
- A regular practice
- Assistance from experienced personnel, who help to carry out the washing
- Variable efficacy
THE ANTIBIOTIC COVERAGE
In the pre-operative period, once the disease is diagnosed, antibiotic drugs are administered. They serve to fight bacterial infections, which, as we have seen, often cause cholesteatoma and foul-smelling otorrhea.
Prognosis and prevention
The prognosis for people with cholesteatoma depends on when the disease is diagnosed and how extensive the cholesteatoma is. In other words, an early diagnosis guarantees a higher success rate of the surgery and a lower chance of relapse.
Conversely, late diagnosis and failure to treat ear infections make the patient more prone to complications, such as meningitis and permanent deafness.
After surgery, the patient should take care to regularly wash the ears (to remove debris and earwax), thereby preventing the formation of another cholesteatoma.