
Usually, this situation is substantially superimposed on a pathological reduction of hemoglobin (Hb) below the reference levels. The result is a lower capacity of the blood to carry oxygen, which results in the characteristic symptoms of anemia.
The causes are numerous; the main conditions that predispose to the onset of microcytic anemia include iron deficiencies, thalassemia and chronic diseases (such as celiac disease, infections, collagenopathies and neoplasms).
Microcytic anemia can be diagnosed by having simple blood tests. The complete blood count and the evaluation of the mean corpuscular volume of red blood cells (MCV) are useful, in particular, to detect the presence of smaller than normal erythrocytes.
Treatment involves several approaches, including iron and vitamin C supplements, diet modification, and more or less recurrent blood transfusions. Sometimes, no therapeutic intervention is necessary.
).
These forms of anemia are usually also hypochromic, ie they are associated with a lower hemoglobin concentration than normal values, for age and sex.
Note
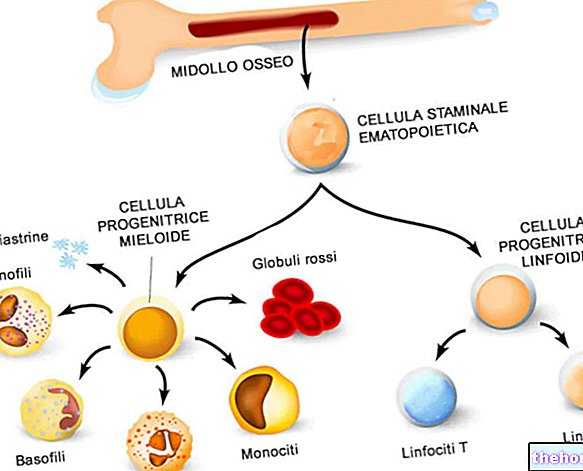
The various forms of anemia can be classified on the basis of the size of the red blood cells and the average concentration of hemoglobin (Hb) contained within them.
Size of erythrocytes: macrocytes, microcytes and normocytes
- Microcytic anemia is characterized by microcytic erythrocytes, that is, smaller than normal; vice versa, we speak of macrocytic anemia.
- If the average concentration of hemoglobin contained within the red blood cells is lower than normal, we speak of hypochromic anemia; when it is higher, we speak of hyperchromic anemia.
Hemoglobin content: hypochromia and normochromia
In addition to microcytosis, anemia can also be associated with a lower concentration of hemoglobin; in this case, we speak of hypochromic microcytic anemia. When the Hb content is normal, but the red blood cells are small, we speak, instead , of normochromic microcytic anemia.
;The role of hemoglobin
Hemoglobin (Hb) is a protein contained within red blood cells, specialized in transporting oxygen to the various parts of the body. In a healthy adult, its concentration should not drop beyond 12 g / dl. "hemoglobin, associated with that of red blood cells in the bloodstream, leads to symptoms that characterize microcytic anemia.
In some cases, the erythrocytes may be smaller due to the presence of genetic mutations that interfere with erythropoiesis, ie in the formation of blood cells; in this case, we speak of hereditary microcytosis.
Microcytic anemia: what are the main causes?
Microcytic anemia can be caused by various conditions and diseases, the main ones being:
- Chronic iron deficiencies:
- Low iron intake;
- Decreased iron absorption;
- Excessive iron loss
- Thalassemia (hereditary alteration in the blood concerning the chains that make up hemoglobin);
- Chronic diseases:
- Chronic inflammatory diseases (eg rheumatoid arthritis, Crohn's disease, etc.);
- Various types of neoplasms and lymphomas;
- Chronic infections (tuberculosis, malaria etc.);
- Diabetes, heart failure and COPD.
- Lead poisoning (substance that causes inhibition of heme synthesis);
- Vitamin B6 (pyridoxine) deficiency.
Rarer forms are congenital sideroblastic anemias (due to deficient synthesis of heme) and some hemoglobinopathies, such as hemoglobinopathy C (due to crystallization of hemoglobin) and hemoglobinopathy E (full-fledged thalassemic syndrome).
.
Depending on the disease that caused it, the microcytic anemia assumes particular characteristics both in the symptoms and in the values found with laboratory analyzes.
In most cases, they manifest themselves:
- Pallor (accentuated at the level of the face);
- Exercise intolerance, premature fatigue, muscle weakness and fatigue;
- Fragility of nails and hair;
- Anorexia (lack of appetite);
- Headache;
- Shortness of breath;
- Dizziness.
In the most severe cases, the following may occur:
- Syncope;
- Palpitations;
- Confusion;
- Chest pains
- Jaundice
- Blood loss and bleeding tendency
- Recurrent attacks of low-grade fever;
- Diarrhea;
- Irritability;
- Progressive distension of the abdomen (secondary to splenomegaly and hepatomegaly).
For a better characterization of microcytic anemia, therefore, it is useful to perform the following blood tests:
- Complete blood count:
- Number of red blood cells (RBC): generally, but not necessarily decreased in microcytic anemia;
- Erythrocyte indices: provide useful information regarding the size of red blood cells (normocytic, microcytic or macrocytic anemias) and the quantity of Hb contained within them (normochromic or hypochromic anemia). The main ones are: Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH) and Mean Corpuscular Hemoglobin Concentration (MCHC);
- Count of reticulocytes: quantifies the number of young (immature) red blood cells present in the peripheral blood;
- Platelets, leukocytes and leukocyte formula;
- Hematocrit (Hct):
- Amount of hemoglobin (Hb);
- Amplitude of Red Cell Volume Distribution (RDW).
- Microscopic examination of the erythrocyte morphology and, more generally, of the peripheral blood smear;
- Sideremia, TIBC and serum ferritin;
- Bilirubin and LDH;
- Inflammation indices, including C reactive protein.
Microcytic anemias are by definition characterized by an average globular volume (or MCV) of less than 80 femtoliters. These anemias are usually also hypochromic, meaning they have a mean globular hemoglobin (MCHC) content of less than 27 pg.
If the iron is low, the microcytic anemia probably depends on an iron deficiency or is secondary to a chronic disease.
orally (or intravenously, when the patient is symptomatic and the clinical picture is severe) and vitamin C (helps to increase the body's ability to absorb iron),The treatment of microcytic anemia can also include:
- Blood transfusions to make up for the lack of red blood cells, possibly associated with a chelation therapy to avoid the accumulation of excess iron;
- Splenectomy (if the disease causes severe anemia or splenomegaly)
- Bone marrow or stem cell transplant from compatible donors.
In addition to specific therapies, regular physical activity and changes in eating habits are of great importance.
In particular, it can be useful:
- Consume foods rich in calcium and vitamin D, due to the risk of osteoporosis (a disease often related to anemia);
- Take folic acid supplements (to increase red blood cell production).
In any case, the doctor will be able to advise the patient on the best interventions to manage their condition. Treatment of the underlying pathologies responsible for microcytic anemia usually results in resolution of the clinical condition.
It should be noted, however, that some forms, such as those caused by thalassemias and some types of sideroblastic anemia, are congenital, therefore they are not curable.




















-nelle-carni-di-maiale.jpg)




