During childhood and adolescence, the bone is interested in continuous processes of renewal and growth, which lead it to reach, around the age of 20-25, the definitive structure in terms of length and strength.
The peak bone mass (PMO) is the amount of bone mineral tissue present at the end of growth; it is reached around 16-18 years for females and around 20-22 for males. During the third decade of life, minimal increases still occur bone mineral content.
From this moment on, bone density and size no longer increase and remain constant throughout adulthood. Despite this, the bone will continue to be the site of a continuous remodeling process, during which the percentage of bone resorbed it will be compensated by an equal amount of newly formed bone. In the elderly, however, this replacement is no longer balanced and resorption prevails over deposition. It is a slow and gradual process that involves both cancellous and compact bone; the result, in many cases, is a disease known as osteoporosis.
If we compare peak bone mass to a bank account, a major capital investment at a young age (through adequate physical activity and diet) will provide enough interest to spend, without running into the red as we get older.
Bone loss begins between 35-45 years in women and between 40-50 years in men; for both it has been estimated at 0.3-1% per year, although in the years around the menopause it can rise to around "1-5% per year" (as a result of the reduced secretion of estrogen by the ovarian tissue).
We can therefore summarize the changes in bone mass in the following stages:
- Growth: from fetal life to puberty
- Consolidation: achieving peak bone mass
- Maturity: maintenance of the achieved bone mass
- Aging: progressive reduction of bone mineral content
Bone mass and osteoporosis
Osteoporosis is a disease characterized by the progressive rarefaction of the bone tissue, which becomes more fragile and susceptible to fractures, especially at the level of the vertebrae and the femur.
A reduced peak in bone mass at a young age increases the risk of osteoporosis in old age, when the protective action of sex hormones (testosterone for men and estrogen for women) decreases.
The introduction of an adequate diet containing calcium and vitamin D positively influences the risk of osteoporosis and the consequent fragility fractures.
The regular practice of physical activity during the adolescent / juvenile period, combined with a balanced diet, rich in calcium, and with an adequate sun exposure, favors the maximum bone mineral development, removing the risk of osteoporosis in old age.
On the other hand, boys who follow a low-calorie diet during adolescence and combine it with excessive physical activity are more exposed to the risk of osteoporosis, already at a young age (see triad of the female athlete).
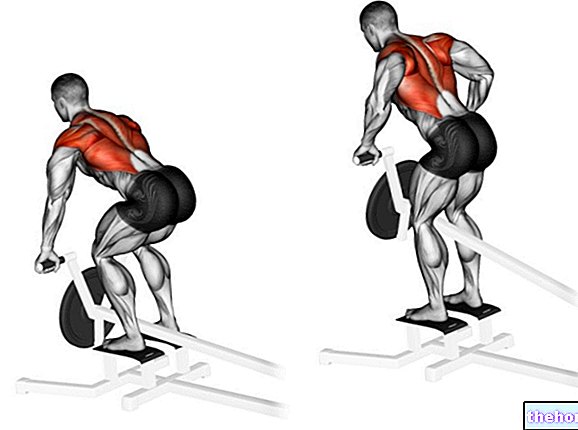
The most suitable form of exercise to increase or maintain bone mass is gravitational (exercise in an upright position that imposes the load on the body weight, such as running and activities that involve it); less effective are exercises performed in unloading, such as swimming or cycling. Athletes practicing power sports generally have a higher bone mass than those who require long-lasting resistance. Probably, this occurs due to the greater muscle mass of the former (more weight = more gravity stimulus), the greater synthesis of anabolic hormones in response to physical activity and other minor elements.
Wollf's law states that bone continuously adapts to varying static and dynamic loads and stresses, remodeling itself in order to respond to functional situations and using the minimum necessary amount of bone tissue.
In other words:
the bone needs stimulation to maintain its shape and density.
It should also be considered that the increase in bone mass is specific to the skeletal site used in the movement. Also for this reason we recommend a physical activity of a global type (multipurpose, multisport, multilateral) during the age of development.
In the case of bed rest and in absence of gravity (astronauts) there is a loss of bone mass.

Note the thicker arrow under the genetic factors, underlining the greater weight of this element on the others. The role of genetics in the variability of bone mineral mass (BMD) between individuals is quantifiable in the 60-70% range.
Physical activity with gravitational load, even of moderate intensity but preferably intense (except for contraindications), is not only important to reach a high peak of bone mass, but also to mitigate mineral loss with aging.
Numerous diseases (hypogonadism, hypercortisolism, thyrotoxicosis, hyperparathyroidism) and prolonged therapy with cortisone, immunosuppressants or thyroid hormones, can weaken the bones; the same goes for lifestyles dotted with alcoholism, smoking and the abuse of caffeine.
Measure bone mass
Today, there are two main instrumental tests that can accurately quantify the bone mass of an individual. Very useful for monitoring the evolution of bone diseases and evaluating the effectiveness of their treatment, they are completely safe, painless and last a few minutes. The first is called DEXA and uses a weak X-ray beam, which is not dangerous for the patient's health. The second uses ultrasound.
Related Topics:
Calcium and bone health
Calcium and osteoporosis
Diet and osteoporosis
Calcium in food
Calcium-rich cheeses
Calcium and phosphorus
Osteoporosis
Osteoporosis in menopause
Physical activity and osteoporosis
Bone decalcification
Other articles on "Bone mass, peak bone mass"
- bone remodeling
- bone
- bones of the human body
- bone tissue
- osteoblasts osteoclasts
- spongy bone compact bone
- periosteum endosteum
- bone marrow
- height growth
- joints
- Joints: anatomy structure