Increasingly, in newspapers and on television, we read and talk about growing overweight, among adults and children, and relative obesity.
To complete this picture, the consequent increase in risk factors for coronary artery disease is exponentially increasing.
However, we do not talk as frequently about how to make a correct diagnosis and especially what to do if the results were positive for a probable adverse cardiovascular event (CVD).
Beyond drug therapy or surgery, the guidelines are completely inadequate and superficial.
Diet therapy and the prescription of physical exercise are the only truly incisive weapons available to combat acute and chronic disorders, but in Italy, to date, there is a frightening scientific and cultural backwardness.
In America the situation is different.
Despite being a country in which there is an "evident contradiction - in fact, obesity and cardiovascular diseases are rampant in the face of world-leading diagnostic and therapeutic programs - the government invests heavily, in proportion to ours, in research and experimentation.
The AACVPR (American Association of Cardiovascular and Pulmonary Rehabilitation), the AHA (American Heart Association) and the "ACSM (American College of Sports Medicine) are the leading authorities that dictate the worldwide guidelines for the diagnosis and treatment of diseases related to CVD and obesity.
According to these organisms, the initial approach with the patient is a moment of fundamental importance.
The anamnesis must be complete, the stratification of risk factors linked to a cardiac or metabolic pathology must be performed thoroughly, all laboratory tests must be consulted, and only then can the evaluation and interpretation of clinical diagnostic tests be carried out.
But let's try to bring these theoretical concepts back to the real dimension with a practical example:
PATIENT:
TO)
Gender: woman
And ty: 48 years old
Ethnicity: white
Family history: premature menopause - sudden death of the father at the age of 52
Smoker: has stopped for 5 months
Pressure: 141/95
Total cholesterol: 195 mg / day
LDL cholesterol: 125 mg / dl
HDL cholesterol: 33 mg / dl
Fasting blood sugar: 116mg / dl
Triglycerides: 280mg / dl
SGOT: 20u / L
SGPT: 12u / L
Urea nitrogen: 15mg / dl
Hematocrit (%): 41
Creatinine: 1.0 mg / dl
Total iron: 100ug / dl
Body mass index: 26.0 kg / m2
Waist circumference: 86cm
Sedentary lifestyle: the patient has not been physically active for about 3 years
Disorders: orthopnea and paroxysmal nocturnal dyspnea - edema in the ankles
Previous diseases: no metabolic or other diseases
B)
Relative or absolute contraindications to the stress test: none
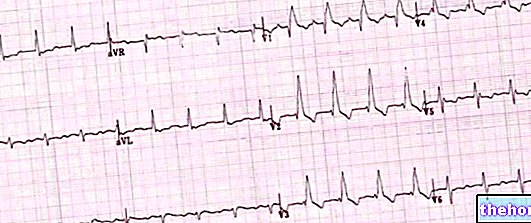
Submaximal diagnostic test: conducted on a moving walkway with adapted single-stage Aåstrand-Ryhming protocol
Inotropic / chronotropic incompetence: absent
Unevenness of the ST segment: absent
Arrhythmias: absent
Angina: absent
Exercise hypo / hypertension: absent
Ataxia or syncope: absent
Cyanosis or pallor: absent
Cramps, dyspnoea, claudication: absent
Pain: absent
VO2 max calculated: 6.7 MET
At first glance, the patient appears relatively healthy: from the haematochemical tests, the anamnesis, the recent disorders and the submaximal diagnostic test there is no evidence of a possible unfavorable event, but looking more carefully at the data we realize which is not the case.
According to the indications of the aforementioned organisms, in fact, the patient presents with 6 risk factors for the development of an atherocoronary and / or metabolic disease, the complained disorders represent a symptom of possible CVD, and her VO2 max is really too much. low, which demonstrates poor functional capacity.
The patient falls into a level B class with stratification of: moderate risk.
Treatment involves lifestyle changes within a maximum of 6 months, prescribing physical activity and diet therapy to reduce risk factors to at least 2, no drug therapy.
For intense physical exercise-> 70% HRmax or> 60% Vo2 max- the presence of health personnel (doctors or nurses) is required, but not necessary for the execution of moderate intensity exercise- <65% HRmax or < 55% Vo2 max-.
The patient / client will be trained no more than 3 times / week and for no more than 35-40 minutes at a time, constantly monitoring the progress of total body water and lean mass, and adapting the training to the results of the examination. of body composition.
The physical exercise will be divided into an initial warm-up, multi-joint exercises with free weights with an intensity between 40-55% of 1RM, fast walking and / or running on a treadmill at an intensity between 45-65% of Variable slope HRmax, cool-down on carpet at 30-40% HRmax.
No increases in muscle endurance or running intensity are expected, at least for the first 3-4 weeks; the subsequent increase in muscle endurance will occur with an increase in repetitions and sets, not in the training load, at least for the first 3 months.
Particular attention is paid to the warm-up and cool-down phases.
"Post-exercise" stretches if the case requires it, and strictly "in chain".
Quarterly follow-up.
For the execution of the submaximal stress test, the supervision of medical personnel is not required - in America, in Italy it is necessary instead for a maximal test.
Diet therapy, assisted by the attending physician, will be set up with a protocol of 5 meals / day with the ratio of macronutrients divided as follows: 60% carbohydrates, 20% proteins, 20% lipids.
The caloric intake is estimated on the total daily metabolism, therefore on the percentage of the patient's lean mass; therefore, an analysis of the body composition is necessary, with monthly follow-up.
The above example of diagnosis and treatment should be the practice, not the exception.
Furthermore, the collaboration between physician and exercise clinician is essential to protect people's health.
To date, in Italy, it is unthinkable that this does not happen!
In summary, metabolic diseases and heart disease are unfortunately on the rise, and the prescription of physical exercise and dietary therapy, combined with drug therapy when the case requires it, are absolutely indispensable for the diagnosis and treatment of these diseases.
Bibliography:
-Steve Glass, Ph.D .: "HFI®-ES®Workshop-Case Studies", American College of Sports Medicine 2005
-G.M. Pontieri: "Pathology and general physiopathology", PICCIN
-Richardson et al .: "Physical activity and Mortality across Cardiovascular Disease Risk Groups",
November 2004 - Medicine & Science in Sports & Exercise®, MSSE®, Official Journal of the American College of Sports Medicine
- Various authors: "Fitness-the complete guide", I.S.S.A. Ed. Club Leonardo
-L.Pescatello, Barry A.Franklin et al .: "Exercise and Hypertension", 2004-Med. Sci. Sports Exerc., ACSM
Other articles on "Heart disease and metabolic disorders"
- Ischemic heart disease - Drugs for the treatment of ischemic heart disease
- Ischemic heart disease
- Coronary heart disease in short
- Ischemic heart disease: pathophysiology