The need to classify the most disparate sports disciplines according to criteria that meet certain purely biological or operational purposes, has clashed from the very first attempts with the objective difficulty of identifying the criteria to be followed. On the other hand, an updated and comprehensive classification represents an important operational tool for the daily work of the specialist in Sports Medicine (MS) and the consultant cardiologist, who must know not only the organs, districts and functions particularly involved in the practice of the various sports disciplines , but also, and equally well, the bioenergetic and biomechanical characteristics that distinguish many sports known and practiced today, with particular reference to the real or hypothetical cardiovascular risk.
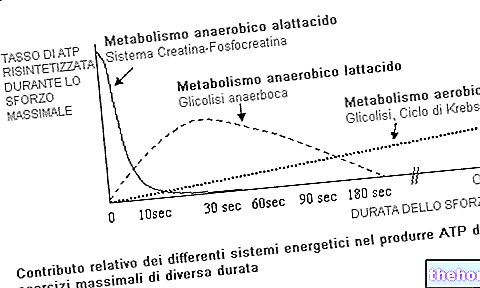
Sports activities, in fact, from the physiological point of view can be classified differently in relation to one or more parameters that characterize them. Thus, a general classification can be made on the basis of the energy sources used in muscular work, anaerobic, alactacid or lactacid, aerobic, and the biomechanical characteristics of the sporting gestures of those activities. This type of approach is still of great use from a strictly physiological and technical point of view, only by feeling the need to appropriately modify the location of those sports specialties in which the greatest progress is made from the point of view of athletic performance and the most sensitive. the technical innovations made.
None of these classifications fully meet the needs of the sports cardiologist, who must specifically take into account the acute and chronic effects that sports activity determines on the cardiovascular system.
It should be emphasized that the objective evaluation of cardiovascular commitment appears to be one of the determining elements in the formulation of the judgment of suitability, especially in athletes with mild heart disease or electrical anomalies, which generally imply a minimum risk or all absent, which can instead become significant as a function of sports practice.
Unfortunately, the reciprocal interrelationships between sports exercise and the cardiovascular system are much more complex than some schematizations carried out so far suggest. This derives above all from the fact that the cardiac commitment in the various activities is extremely variable in relation not only to the factors of the chosen sport, but also to contingent external factors (psychic state of the athlete, atmospheric conditions, etc.). Furthermore, it must be taken into account that cardiac commitment can be constant over time, as practically occurs in long-term competitions (marathon, cross-country skiing, cycling, etc.) or intermittent, as occurs for example in ball games (aerobic activity alternating anaerobics), without this significantly diversifying the two types of sports activities in terms of cardiovascular risk. arrhythmogenic potential compared to efforts, albeit maximal, but started and ended gradually. To confirm this, an abrupt stop after heavy, dynamic, static or mixed efforts often appears to be much more perturbative from the haemodynamic and arrhythmic point of view than any other condition typical of sporting activity.
In sports with a prevalent neurosensory involvement, the cardiac component may appear modest from the haemodynamic point of view and is instead remarkable in terms of neurohormonal stress, especially catecholaminic, even if the latter alone is probably not sufficient to realize a real heart risk if not in exceptional cases.
A not negligible aspect is represented by the intrinsic risk of certain sports activities in relation to the unfavorable environment in which they take place (underwater sports, mountaineering, motor sports, etc.). In these disciplines, the possible onset of syncopal episodes with genesis arrhythmic and hemodynamics can be much more dangerous for the athlete and possibly for the spectators (motor sports). From this same point of view, albeit in probabilistic terms, it is reasonable to assume that cardiovascular risk may increase in contact sports in which it is possible to develop contusive thoracic trauma or violent reflex cardiac stimulations (head trauma, intense algogenic stimulations) capable of facilitating the onset of arrhythmic phenomena, mostly of the hypokinetic type.
While taking into account all the above difficulties, a classification of sports activities that takes into account the cardiovascular commitment is still an essential tool to facilitate and rationalize the work of the Sports Physician and the consultant cardiologist.
Completely recently new and more complex needs have emerged, largely referring to modern training schemes or linked to the modifications of motor commitments that have occurred in recent years both for tactical reasons and because made possible by the greater potential that athletes are today. able to express, thanks also to modern training techniques. Added to these reasons is the continuous emergence of new sports disciplines, some of which have already been recognized by the National Sports Federation.
Furthermore, technological and scientific progress has made it possible to acquire new information and to modify some concepts acquired in previous classifications. For example, concepts such as "isometric commitment, static commitment and dynamic commitment" are misleading as "static or isometric" loads have now almost disappeared and in competition the "static or isometric" phases can only occur in rare episodes and for a very few seconds or fractions of a second, however not able to produce significant overloads on the cardiovascular system.
From what has been described so far, the need to proceed with a review of sports activities that takes into account the cardiovascular commitment clearly emerges.
In particular, for practical purposes, easy-to-detect parameters such as heart rate, pump load, working pressure and emotional influences were used as the guiding criteria of the classification. In fact, these parameters allow, if correctly used, to be formulated by the specialist in M.S. and from the consultant cardiologist a reliable judgment regarding the assessment of cardiovascular risk.
Furthermore, in dividing the various sports within the classification, it was deemed necessary not to limit oneself to considering only the cardiovascular commitment of the race but also that of training, much more incident, both in terms of intensity and quantity, on the haemodynamic risk. The evaluation of the workload in training is obviously difficult, varying from sport to sport and from coach to coach; however, the most common acquisitions in these sectors deriving from the literature or from experimental data were taken into account. On the basis of this classification criterion it will therefore be possible to verify that sports that could be classified, for the competition load, among those with moderate commitment, are instead included among those with high commitment for what athletes perform in training.
Evidently this classification too has, due to the intrinsic limits of each classification, only an indicative character.
Curated by: Lorenzo Boscariol
Other articles on "Sports activities and cardiovascular commitment"
- competitive fitness
- cardiovascular system
- athlete's heart
- cardiological examinations
- cardiovascular pathologies
- cardiovascular pathologies 2
- cardiovascular pathologies 3
- cardiovascular pathologies 4
- electrocardiographic abnormalities
- electrocardiographic abnormalities 2
- electrocardiographic abnormalities 3
- ischemic heart disease
- screening of the elderly
- cardiovascular commitment sport 2 and BIBLIOGRAPHY

















.jpg)