This type of ulceration generally has a rounded shape and is attributable to the corrosive action of the acidic gastric juices produced by the stomach itself.
.Gastric ulcer appears more frequently in the lower social classes, but it is not clear whether this is linked to particular dietary factors or risk behaviors, such as smoking, coffee intake, emotional stress or the use of non-steroidal anti-inflammatory drugs (so-called NSAIDs).
normal or slightly below normal; for this reason the most accredited hypothesis is that of a decrease in the resistance of the gastric mucosal barrier to the aggressive action of the acid-peptic secretion.
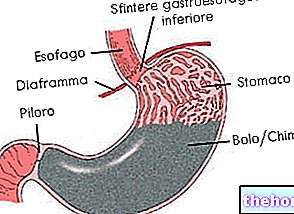
The gastric juices produced by the stomach have digestive and defensive functions against pathogens that enter the digestive tract and are very corrosive; for this, some specialized cells of the stomach (superficial mucous cells) produce a layer of mucus - containing proteins and bicarbonates - to protect the gastric mucosa. The protective action of the mucus is carried out by maintaining a higher pH value in the mucosa than that of the gastric secretion; thus a barrier is created that prevents the acid from damaging the mucosa and submucosa. Furthermore, the rapid turnover of the epithelial cells of the stomach guarantees the rapid repair of any lesions caused by the aggressive action of the gastric juice. All the factors that are considered responsible for the onset of gastric ulcer are able to alter this protective barrier. increase gastric acidity or hinder the natural repair processes of the mucosa.
In the stomach of patients suffering from gastric ulcer, alterations typical of gastritis (inflammation of the mucosa) are always found. The onset of gastritis always precedes that of the ulcer and the mucous membranes involved in gastritis have a reduced capacity of secretion of bicarbonate in the mucus; this explains the onset of the ulcer.
Gastric ulcer and rising bile
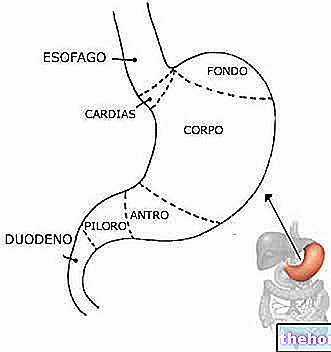
Chronic antral gastritis (of the pyloric antrum) is perhaps the condition whose correlations with the onset of gastric ulcer are best known. It is due to the presence of reflux from the duodenum to the stomach, following which a high quantity bile (which is secreted in the duodenum) comes into contact with the gastric mucosa. Being a weak acid, it neutralizes the secretion of bicarbonate in the stomach.
Gastric ulcer and Helicobacter pylori
In 50-65% of patients with gastric ulcer there is the presence at the level of the "pyloric antrum"Helicobacter pylori, a bacterium that is located below the mucosa. L"Helicobacter pylori it is able to induce a local inflammatory reaction that triggers a response of the immune system which, in turn, makes the mucous lining more vulnerable to the attack of gastric juices, thus favoring the lesion of the epithelial cells of the mucosa itself.
Gastritis from Helicobacter pylori it could therefore represent a predisposing factor to the onset of the stomach ulcer.
Gastric ulcer, diet, drugs and behavioral factors
Numerous external, dietary and behavioral factors can facilitate the onset of gastric ulcer. For example, non-steroidal anti-inflammatory drugs (NSAIDs) are gastrically injurious, reduce the concentration of bicarbonate in the mucus and inhibit the synthesis of prostaglandins, molecules that exert a "protective action on the gastric mucosa. Corticosteroids also exert a" damaging action against the mucosa, possibly altering its blood flow.
Alcohol, ingested in high quantities, reduces the bicarbonate content of the mucus, although there is no solid evidence of increased incidence of gastric ulcer in alcoholics.
Caffeine can dramatically increase gastric acid production; while the fats of the diet are able to decrease the resistance of the mucosa to acid aggression, probably by depressing the secretion of bicarbonate in the mucus.
Cigarette smoking slows gastric emptying and increases reflux from the duodenum to the stomach, as well as reducing the secretion of bicarbonate.
Thus, the increased frequency of peptic ulcer may be the result of risky eating and living habits, such as smoking and coffee abuse and dietary disorders.
Genetic predisposition and psychological factors
In the development of gastric ulcer there is also a certain genetic predisposition: a higher incidence of the disease is found in subjects of blood group 0.
Psychological factors also seem to play a significant role in the onset of gastric ulcer: individuals with fragile and dependent personalities, or exposed to situations of high conflict and strong stress, develop gastric ulcer with a higher frequency.
; 85% of them are located along the lesser curvature of the stomach, while the remaining 15% are distributed on the anterior and posterior wall and along the greater curvature.The macroscopic appearance of benign gastric ulcer is that of an excavated lesion, round or oval, usually less than 2 cm in diameter, which arises on inflamed mucosa due to gastritis. At the bottom of the ulcer can sometimes be found vessels with blood clots or signs of a small bleeding in progress.
The depth of the ulcer is variable: it can barely exceed the muscularis mucosae or it can reach the serosa and even exceed it, causing a free perforation in the peritoneum or deepening into nearby organs adhering to the stomach, such as the liver and pancreas.
and heartburn located in the upper and middle region of the abdomen. It is often a dull, cramp-like pain, sometimes described as a sense of pressure, heaviness or emptiness in the stomach.Pain, of varying intensity, typically occurs within the first 30 minutes after a meal (early postprandial pain). In ulcers located along the small curvature, antacids provide prompt relief of pain, while food, after a temporary well-being, can even induce a flare-up.
Nausea and vomiting may also be present. 40% of those suffering from gastric ulcer report a decrease in body weight of variable entity, linked to the aversion for food induced by the disorders.
A seasonal periodicity can be added to the periodicity of the painful symptoms throughout the day, with characteristic accentuations in the spring and autumn period.
An aggravation of symptoms can also occur as a result of sudden changes in eating or working habits, or after periods of psycho-physical or emotional stress.
The presence of non-periodic pain or of rapid and sudden changes in the classic symptoms must lead us to suppose the onset of complications or the non-peptic, but rather neoplastic, nature of the gastric ulcer.
Finally, it should be remembered that in some patients, gastric ulcer does not give rise to any symptoms.
For further information: Gastric Ulcer Symptoms. These haemorrhages occur when the ulcer, becoming sufficiently deep, erodes the blood capillaries. The possible haemorrhagic complication can become evident with the emission of dark, tarry stools, or with the appearance of blood vomit or similar material. coffee grounds.
In severe cases, gastric ulcer can cause occlusions due to tissue scarring. While in extreme cases, fortunately rare, the lesion can also extend through the entire thickness of the stomach wall, perforating it. A perforated gastric ulcer is extremely dangerous. , as the acidic contents of the stomach can leak into the peritoneal cavity, causing severe damage. In these cases, sudden epigastric pain may occur, followed by signs and symptoms of acute abdomen (very severe stabbing pain, such as a stab, hard abdomen, nausea, vomiting, sweating, tachycardia, weak pulse and assumption of the curled up position. side).
Both digestive bleeding and perforated ulcer always require immediate medical-surgical treatment. Therefore, pay attention to warning signs, such as the appearance of intense, sudden and persistent stabbing pain in the stomach.
, gastritis, duodenitis, duodenal ulcer, gallbladder stones or chronic inflammation of the same; particularly important is the differential diagnosis with stomach cancer.The diagnosis of gastric ulcer is hypothesized on the basis of symptoms and confirmed by instrumental tests, such as gastroscopy and radiographic examination with contrast medium.
Gastroscopy is considered as the first choice diagnostic approach; the direct visualization of the ulcer makes it possible to evaluate its size and shape, as well as to perform sampling (biopsy). On these biopsies, in addition to the "histological examination, also the research of the"Helicobacter pylori. The presence of a "possible infection with Helicobacter pylori it can also be detected by a blood or stool test, or by a test known as a urea breath test.
The radiological examination is performed with a baryte meal, that is, marked with a fluorescent substance so that it can be seen on X-rays. According to the rapidity or otherwise of the passage of the contrast medium, the gastric emptying time and others can be evaluated. parameters.
and histamine H2 receptor antagonists. In addition, if the ulcer is associated with Helicobacter pylori It is also associated with antibiotic therapy capable of eradicating the infection. Finally, in the most serious cases, surgery may be necessary to repair the damaged tissues.
Prevention of Gastric Ulcer
To prevent the onset of gastric ulcer it may be useful:
- Adopt a dietary regime that excludes drinks and foods that increase acid secretion, such as, for example, coffee, tea, chocolate, mint, carbonated soft drinks, pepper, spices, etc.
- Minimize, or even better avoid, the consumption of alcohol.
- Pay attention to the prolonged use of anti-inflammatory drugs; in any case, these drugs should always be taken following the doctor's instructions.
- Stop smoking.
Other articles on "Ulcer"
- Peptic ulcer
- Duodenal ulcer
- Peptic ulcer therapy
- Medicines to Treat Ulcer
- Ulcer: herbal medicine and natural remedies