Heartburn is the term with which doctors identify the unpleasant sensation of discomfort, or burning pain (burning), felt behind the breastbone with a tendency to radiate towards the throat (sense of acidity rising).

Heartburn is a fairly common symptom, which occurs in numerous circumstances. This annoying burning can in fact appear at any time, but is more common about half an hour after a meal or at a long distance from it; it is often associated with dyspepsia (indigestion) and in this case it is typically accompanied by nausea, belching and regurgitation. Furthermore, heartburn disturbs the sleep of many people, since the ascent of gastric juices in the esophagus is favored by the lying position; for the same reason, this symptom can also appear during particular movements of the trunk, such as the act of lacing the shoes or pick up an object from the ground. Finally, it is now well established that the onset of heartburn, or at least its aggravation, are often related to emotional factors.
Beyond the single and isolated episodes of heartburn, experienced firsthand by the majority of individuals, the repeated onset of this symptom tends to assume pathological connotations. In most cases, in fact, this symptom indicates gastroesophageal reflux, a condition characterized by the "abnormal rise of the acid content in the" esophagus. The underlying causes of this reflux can be multiple and overlapping: incontinence of the gastroesophageal sphincter, hiatal hernia and changes in the tone of the esophageal or gastric muscles are the most common causative agents.
Esophageal spasm, sudden dilation and spastic contraction of the lower esophageal sphincter
Scleroderma
Gastritis
Peptic ulcer
Neoplasms with secondary impairment of sphincter function
Gastro-injuring drugs (for example NSAIDs, such as aspirin and ibuprofen, some sedatives and some antihypertensives)
Coffee (decaffeinated is better) and other caffeinated drinks
Carbonated or particularly hot drinks
Foods such as onions, tomatoes, sour sauces, citrus fruits, chocolate, spirits, mint, and particularly fatty or spicy foods.
Overweight or Obesity.
Go to bed or perform physical activity shortly after a meal.
Stress, depression, anxiety and hypochondria.
Aerophagia (typical of those who eat meals too quickly or talk a lot while eating).
Pregnancy
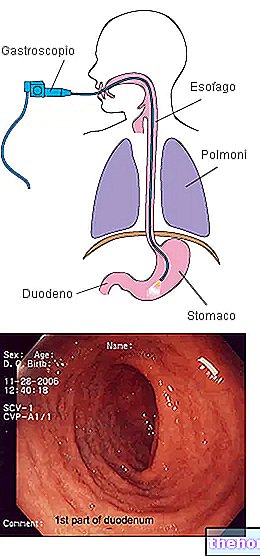
The diagnosis of reflux disease is predominantly clinical. Doctors usually only diagnose GERD after ruling out other pathological conditions, such as heart problems or a hiatal hernia. If these findings are negative and the symptoms persist, therapy with antacid drugs is initiated. If the patient's response to these drugs is positive, further tests are not usually necessary. If, on the other hand, the symptoms persist or reappear at the end of the therapy, it is advisable to perform further tests, using instrumental investigations such as "esophagus-gastroduodenoscopy, pHmetry, esophageal manometry and biopsy (to ascertain the" absence of complications, such as for example " Barrett's esophagus).

The intake of drugs with antacid action is generally sufficient to resolve the heartburn symptom. For this purpose, common over-the-counter antacids (sodium bicarbonate, calcium carbonate, aluminum or magnesium hydroxide), H2 receptor antagonists can be used histamine, alginates or more modern proton pump inhibitor drugs. The preventive intervention of heartburn through behavioral and dietary rules (see diet and gastroesophageal reflux) is fundamental before moving on to pharmacological treatment or in any case attaching it to it.











.jpg)