Generality
Depending on the sources consulted, we speak of fetal macrosomia when the birth weight is greater than 4 kg or 4 kg and a half.
More correctly, the fetal weight should be related not so much to absolute values, as to the standards considered normal for its development; hence, from this point of view, any fetus with a weight greater than the 90th percentile of reference for gestational age is defined as macrosomal.

It must be said, however, that before birth the estimate of the fetal body weight, performed mainly by ultrasound (ultrasound), is quite inaccurate.
Causes
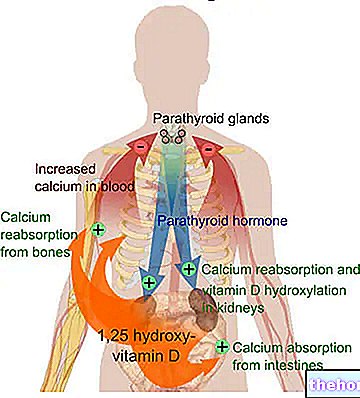
Approximately eight out of 100 infants of nondiabetic mothers are macrosomic; in the diabetic population, on the other hand, the incidence rises to 26%. Diabetes, in fact, represents the main risk factor for neonatal macrosomia, regardless of whether it occurs before or during gestation (gestational diabetes). above all, hyperinsulinemia represent an important element of stimulation of fetal growth. The newborn is thus macrosomic, with organomegaly characterized by larger and more numerous cells than those of normal-weight newborns.
Other important risk factors for macrosomia include obesity, excessive weight gain during pregnancy, multiparity, a previous pregnancy with fetal macrosomia (the condition can still occur even if it did not occur in previous gestations) , ethnicity (the incidence of macrosomia is higher in the black population), family history (a macrosomal child is more likely to be born when family members are tall and robust) and duration of pregnancy (when it lasts beyond 40 weeks, the risk increases In addition, male infants tend to be heavier than females.
Risks for the newborn
In most cases, a macrosomal infant is healthy and healthy. The unborn child can have serious complications if diabetes pre-dates pregnancy and is not adequately controlled. On the contrary, when diabetes arises during gestation (gestational diabetes) - by virtue of the fact that it appears when the development of organs and systems is now completed - it does not cause congenital malformations. It is clear that even a diabetic woman can carry out a pregnancy with serenity and without any complications, but it is essential that conception is preceded by a preventive medical consultation and optimal control of diabetes before, during and after pregnancy. Conception and the very first weeks of gestation, in particular, must take place in a situation of perfect glycemic control.
At the time of birth, for obvious reasons, a macrosomal newborn encounters more difficulty in coming to light naturally, requiring in many cases the use of a caesarean section. In the case of natural birth, therefore, the mother's risks of vaginal laceration (up to the anal sphincter) and post-partum haemorrhages increase, while the unborn child runs a greater risk of fracture and shoulder dystocia. moreover, the unborn child can suffer a hypoglycemic crisis, since - being used to living in a hyperglycemic environment - he can suffer from the sudden decrease in sugars at the moment of detachment of the umbilical cord. Other possible complications at birth are represented by "hyperbilirubinemia and from respiratory distress syndrome.
Macrosomia, like the opposite condition, seems to increase the risk of obesity and its late complications (type II diabetes, atherosclerosis, hypertension) in childhood and later age groups.
Prevention
To prevent macrosomia in diabetic women, an appropriate pre-conception consultation associated with optimal diabetes control before, during and after pregnancy is essential; the pregnant woman, on her part, must strictly follow the recommendations of the pediatrician and the diabetes team, which includes doctors, nurses, nutritionists and social workers.
As for euglycemic women, however, it is very important to prevent the onset of diabetes during the gestational period. This very important preventive work is carried out first of all by regularly discussing with the gynecologist and other assistants. The fundamental recommendations are to forget the old man. said "in pregnancy you have to eat for two" and the increasingly widespread tendency to put purely aesthetic concerns before the well-being of oneself and the unborn child. Respect for advice on nutrition and on the right amount of momentum is essential for the prevention of neonatal macrosomia . A correct dietary-behavioral approach allows in fact to keep blood sugar and body weight within the limits considered "optimal" for pregnancy. In the event that glycemic levels remain high anyway, small doses of insulin may be prescribed with meals.





.jpg)