Generality
Breast engorgement is a typical problem of the first days after birth. It is characterized by the stagnation of milk in the breast, which appears tense, edematous and shiny, sometimes red and painful, however unable to emit significant quantities of milk.
Main causes of breast engorgement:
- Excessive milk production.
- Delay in the initiation of breastfeeding after childbirth.
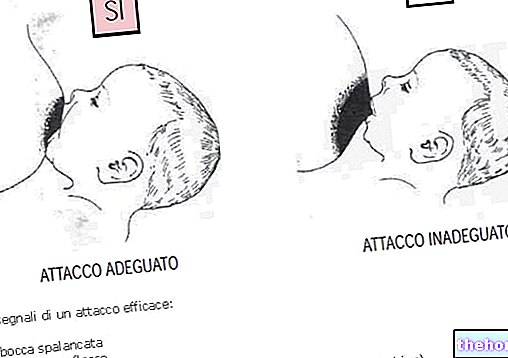
- Inadequate attachment to the breast by the baby.
- Infrequent removal of milk from the breast.
- Overly strict limits on the duration of feedings.
- Bra too tight or clothes that are too tight to the chest.
Signs and Symptoms
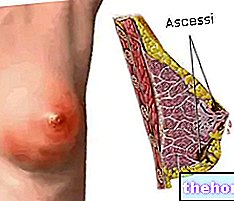
Often, breast engorgement is associated with a slight feverish rise, for about 24 hours; consistent increases in body temperature are instead attributable to a complication, mastitis, characterized by an "infection of the mammary gland with the appearance of malaise, circumscribed abscess and high fever.
A breast may appear hot, heavy and tight simply because it is full of milk; the most important aspect of breast engorgement, in fact, does not concern so much the appearance of the breast, but rather the difficulty in getting the milk out
. The consequent increase in breast tension is such as to reduce the protrusion of the nipple, making the attachment of the baby more difficult and traumatic.
An insufficient sucking, moreover, aggravates the mammary engorgement, increasing the stagnation of milk in the gland and - in the long run - reducing the production of the same by the female organism.
Causes
After childbirth, the onset of milk rising is accompanied by a greater flow of blood and lymph to the breasts, which become swollen, hard, hot, heavy and hypersensitive, if not even painful.

Breast engorgement during the first days of breastfeeding is therefore the result of the increased blood flow into the breast tissue, dictated by the need to support milk production. To prevent breast engorgement in the very early periods of breastfeeding, it is therefore important to latch the baby to the breast within hours of delivery.
In later stages of breastfeeding, breast engorgement can occur when the baby takes less milk than usual, takes too long between feeds, or latches on to the breast inadequately.
Prevention
As stated so far, one of the most common advice given to nurses subject to such problems is to make the baby breastfeed more often, without imposing strict limits on the duration of the feedings.
Another typical advice to resolve breast engorgement is to perform - in the 10-15 minutes before feeding - hot-moist sponging of the breast, or apply warm compresses. In this regard, in this document, the pediatrician Duccio Parrini describes the "interesting" ploy "of the hot bottle.
After feeding, especially if the pain is intense, it is useful to apply cold compresses under the armpits.
Before attaching the baby, it is advisable to use manual expression, releasing modest quantities of milk, to spread on the nipple to soften the areola and favor the attachment of the baby. Only when the mother produces excessive quantities of milk, so that not even frequent sucking reduces the discomfort, or when it is not possible to attach the baby often, is the use of a breast pump recommended.
During the feeding, the breast massage through delicate concentric movements in the direction of the nipple further facilitates the milky outflow.
At the end of the feeding, if the woman still feels a sense of fullness and tension in the breast, the milk can be expressed manually, but without exaggerating, in order to avoid an excessive stimulus to the production of milk.
Finally, allowing yourself a lot of peace of mind during breastfeeding is equally useful in preventing breast engorgement.