Due to the mutation of the NSD1 gene, Sotos syndrome is a condition acquired during embryonic development, in more than 90% of cases, and a hereditary condition, in the percentage of remaining cases; therefore, it is almost always the result of a new mutational event.
The symptoms and signs of Sotos syndrome can be seen, in part, already at birth, which makes early diagnosis possible.
Unfortunately, currently, those suffering from Sotos syndrome can only count on symptomatic treatments - that is, aimed at relieving the symptoms - as there is no cure capable of canceling the consequences of the mutation in the NSD1 gene.
Other names of Sotos syndrome
Sotos syndrome is also known as brain gigantism (referring to) or Sotos-Dodge syndrome.
Epidemiology
According to statistics, one in every 10,000-14,000 individuals is born with Sotos syndrome.
fertilized the egg and embryogenesis began) and, only in the remaining 5-10% of clinical cases, hereditary (ie transmitted by parental route).Thus, Sotos syndrome is, in 90-95 cases out of 100, a condition resulting from a "new" mutation and, in only 5-10 cases out of 100, a condition inherited from the parents.
What causes the gene mutation associated with Sotos syndrome?
Premise: the genes present on human chromosomes are DNA sequences that have the task of producing fundamental proteins in biological processes essential to life, including cell growth and replication.
In the absence of mutations in it, the NSD1 gene produces a protein of the group of histone methyltransferases, whose function is to regulate the activity of genes involved in the processes of growth and development, avoiding cellular hyperproliferation phenomena.
More simply…
In healthy people, NSD1 produces a protein that finely controls the activity of a number of genes involved in the growth and development of the human body.
In the presence of the mutation responsible for Sotos syndrome, the NSD1 gene loses part of its regulatory capacity against the aforementioned genes (NB: the loss is due to a quantitative decrease in NSD1) and this leads to an "abnormal expression of the latter" with repercussions on body and mental development.
More simply…
If mutated, NSD1 is low and this involves an "anomalous activity on the part of the genes under its control, which in turn follows an" alteration of physical and mental development.
Sotos syndrome is an autosomal dominant disease
To understand...
Each human gene is present in two copies, called alleles, one of maternal origin and one of paternal origin.
Sotos syndrome has all the characteristics of an autosomal dominant disease.
A genetic disease is autosomal dominant when the mutation of a single copy of the gene that causes it is sufficient to manifest itself.
To this, it is important to add that the impact of Sotos syndrome on skeletal growth also affects bone aging: compared to their healthy peers, children with Sotos syndrome demonstrate a bone age that is 2-4 years higher.
DOES EXCESSIVE GROWTH HAVE AN END?
The most important effects on skeletal growth by Sotos syndrome end around 3-4 years of life. From this age onwards, in fact, the high rate of skeletal growth gradually tends to diminish, up to normality.
CONSEQUENCES IN ADULT AGE
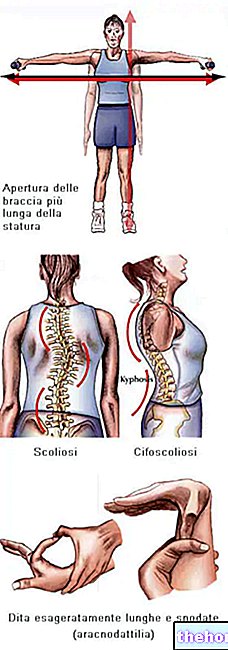
Due to excessive skeletal growth at a very young age, individuals with Sotos syndrome reach, in adulthood, a height of no less than 193 cm.
It is interesting to point out to readers that the weight of these subjects is in line with the weight of healthy individuals of equal height; this means that Sotos syndrome affects only the height and not the body weight.
Craniofacial anomalies
Craniofacial anomalies related to Sotos syndrome are:
- Prominent forehead;
- Receding hairline
- Dolichocephaly (i.e. long, narrow head);
- Abnormally wide apart eyes (ocular hypertelorism);
- Pointed chin;
- Eyelid slits pointing downward;
- Narrow palate;
- Long and narrow face.
The above anomalies are particularly evident at birth; then, with growth, they tend to "fade", to be less visible. The only stable craniofacial signs even in adulthood are: prominent chin, dolichocephaly, prominent forehead and receding hairline.
Delay in intellectual development
In Sotos syndrome, the delay in intellectual development is the consequence of a problem in the central nervous system.
To reveal this intellectual delay are: a certain slowness in learning to speak, language problems (eg: stuttering, problems with sound reproduction, monotonous voice, etc.) and a reduced IQ (stable for life).
Did you know that ...
For 80-85% of patients with Sotos syndrome, the IQ is just over 70 (therefore 30-40 points below normal); for the remaining percentage, however, it is normal.
Delay in motor development
In Sotos syndrome, delayed motor development is manifested by:
- Difficulty walking on all fours (it is clearly a problem of very young age);
- Muscle hypotonia;
- Clumsiness and coordination difficulties (for example, it is difficult to learn to ride a bicycle);
- Motor problems due to poor control of the striated muscles.
With the exception of the first, all the other manifestations mentioned above tend to be maintained throughout life.
Behavioral problems

The typical behavioral problems that can be seen in patients with Sotos syndrome are: attention deficit hyperactivity disorder (ADHD), various types of phobias, aggression, impulsivity, irritability and obsessive-compulsive disorders.
Other symptoms
Sometimes, to the symptomatology reported above - which represents a classic symptomatology - Sotos syndrome can add another series of important clinical consequences, which are:
- Jaundice (especially at birth)
- Inability to feed (especially at birth)
- Epilepsy;
- Loss of hearing;
- Scoliosis (in about 40% of patients);
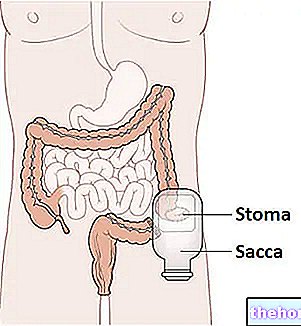
- Malformations of the kidneys and / or urinary tract (in about 20% of patients);
- Heart defects (in no more than 35% of patients);
- Vision problems, such as squinting
- Predisposition to the development of respiratory infections;
- Predisposition to the development of malignant tumors.
Medical history and physical examination
Anamnesis and physical examination essentially consist in an accurate evaluation of the symptoms exhibited by the patient.
In the context of Sotos syndrome, it is in these phases of the diagnostic process that the doctor ascertains the presence of cranial and facial anomalies, abnormal skeletal growth, impaired intellectual development, delay in motor development and any other less common manifestations. .
Radiological examinations
Radiological examinations are used to detect and analyze any abnormalities that may affect the urinary tract, heart or spine (scoliosis).
Genetic test
It is the DNA analysis aimed at detecting mutations in critical genes.
In the context of Sotos syndrome, it represents the confirmatory diagnostic test, as it allows to highlight the NSD1 mutation.
When is the diagnosis made?
Sotos syndrome is diagnosable from birth.
It should be noted, however, that none of the routine examinations, performed in the prenatal phase, allow us to identify the disease in question; for the prenatal diagnosis of Sotos syndrome, in fact, a prenatal genetic test is needed (after an "amniocentesis or a CVS).

- Logotherapy (or language therapy) to stem language disorders;
- Physiotherapy to relieve movement problems;
- A drug therapy ad hoc, aimed at managing ADHD (if any) and / or any other behavioral problems;
- The use of corrective glasses (if there are vision problems);
- Pharmacological or surgical therapy focused on controlling any heart and / or urinary tract problems;
- The implementation of a program of screening oncological, aimed at the timely identification of any malignant tumors (remember that Sotos syndrome favors neoplastic processes).
What medical figures does the symptomatic therapy of Sotos syndrome involve?
The symptomatic treatment of Sotos syndrome requires the coordinated intervention of several medical specialists, including: pediatricians, geneticists, endocrinologists, neurologists, speech therapists, orthopedic surgeons, ophthalmologists, psychiatrists and physiotherapists.