Myocarditis is an "inflammation of the heart muscle.

Myocarditis can be caused by a variety of factors, including infections, systemic diseases, autoimmune mechanisms, exposure to toxins, or hypersensitivity responses to certain drugs.
In many cases, inflammatory myocardial disease produces no noticeable symptoms. However, a severe clinical picture can be associated with:
- Abnormalities of the normal heart rhythm (arrhythmias);
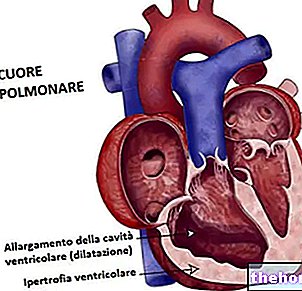
- Weakness of the heart muscle (heart failure: the heart is no longer able to develop the necessary strength to maintain normal range);
- Electrical and / or mechanical dysfunctions of the heart muscle characterized by progressive degeneration of the myocardium (cardiomyopathy);
- Sudden cardiac arrest.
In some situations, the disease can induce necrosis (death) of the heart tissue.
The pathophysiology of myocarditis is characterized by dysfunctions of myocytes (the cells of the myocardium), due to both direct tissue injury and immune-mediated damage.
In most patients, the clinical course is self-limited and myocardial inflammation resolves without permanent consequences. More severe cases, or those that become chronic, may require hospitalization and adequate treatment, which depends primarily on the underlying cause.
Causes
Myocarditis recognizes several causes:
- Viral infections. The most common cause of myocarditis is a "viral infection of the heart muscle. Viruses invade the myocardium and cause" local inflammation with activation of the immune system; this host defensive response attenuates viral replication and protects myocytes from virus-mediated injury. However, some components of the immune reaction may also contribute to the development of myocardial inflammation, necrosis, and ventricular dysfunction. In fact, during and after viral infection, the immune system can attack cardiac myosin and inflict damage to the myocardium (some pathogens have epitopes that are immunologically similar to cardiac myosin). This immune response helps to establish the clinical picture of myocarditis.
Several viruses can cause inflammatory myocardial disease, including: adenovirus, parvovirus B19, coxsackievirus, enterovirus, HIV, Epstein-Barr virus, rubella virus, poliovirus, cytomegalovirus, varicella-zoster virus (HHV-3), and human herpesvirus 6 (HHV-6). - Bacterial infections. In some people with diphtheria, a toxin produced by the Corynebacterium diphtheriae causes a form of myocarditis that makes the heart muscle flaccid and enlarged. As a result of this disease process, the heart cannot pump blood efficiently and severe heart failure can develop within the first week of the disease. Also an "infection caused by the bacterium Borrelia burgdorferi, the causative agent of Lyme disease can cause myocarditis.
Bacterial myocarditis can also be caused by pathogens such as: Brucella, Leptospira, Neisseria gonorrhoeae, Haemophilus influenzae, Actinomyces, Tropheryma whipplei, Vibrio cholerae And Rickettsia. Rarely, myocarditis is a complication of "endocarditis," an infection of the heart valves and the inner lining of the heart's chambers, often caused by bacteria. - Chagas disease. Myocarditis can be caused by protozoan infection Trypanosoma cruzi, transmitted by an insect bite. The pathogen causes Chagas disease, endemic to Central and South America. After the first infection, about one third of affected patients develop a form of chronic (long-term) myocarditis. This leads to a significant destruction of the heart muscle, leading to progressive heart failure, including the protozoan Toxoplasma gondii, responsible for toxoplasmosis can participate in the etiology of myocarditis.
- Inflammatory diseases. These include systemic lupus erythematosus, sarcoidosis and other autoimmune diseases, such as scleroderma and systemic vasculitis (example: Churg-Strauss syndrome and Wegener's granulomatosis).
- Toxic substances:
- Alcohol abuse;
- Heavy metals, chemicals and toxins (example: hydrocarbons, carbon monoxide, toxic shock syndrome, arsenic or snake venom);
- Some drugs: doxorubicin (or adriamycin), anthracyclines, chemotherapy and antipsychotics (for example: clozapine).
- Physical agents: electric shock, hyperpyrexia and radiation exposure.
Other possible causes of myocarditis include rejection after a heart transplant.
About 6-10% of cases of dilated cardiomyopathy are secondary to myocarditis.
Myocarditis can affect people of all ages and, because it is often asymptomatic, can only be diagnosed after a young adult with heart damage from chronic myocarditis dies unexpectedly during exercise (nearly 20% of sudden deaths among young adults and athletes are the consequence of myocarditis).
Potential causes of myocarditis
- Viral infections: adenovirus, coxsackievirus, cytomegalovirus, HIV and parvovirus B19;
- Drugs: anthracyclines;
- Mephedrone;
- Ethanol.
- Autoimmune diseases: Churg-Strauss syndrome, inflammatory bowel disease, Kawasaki disease, systemic lupus erythematosus;
- Bacterial, fungal and parasitic infections;
- Heavy metals: copper, iron and lead;
- Hypersensitivity reaction to: cephalosporins, diuretics, penicillin, phenytoin, sulfonamides and tetracycline.
Symptoms
For further information: Myocarditis Symptoms
The signs and symptoms associated with myocarditis are manifold and depend both on the actual inflammation of the myocardium and on phenomena secondary to the inflammatory process, such as the weakening of the heart muscle.
In mild cases, myocarditis can be asymptomatic and the patient may experience a sense of discomfort and general symptoms, without realizing that the heart is involved. The only sign of heart inflammation may be a temporary abnormal result on an electrocardiogram (ECG), which measures the electrical activity of the heart and demonstrates certain abnormalities, such as decreased strength of heart muscle contractions.
In severe cases, the signs and symptoms of myocarditis vary depending on the cause of the disease. These can include:
- Fever (especially when myocarditis is of infectious origin);
- Chest pain (often described as "stabbing");
- Heart arrhythmias (irregular heart rhythm, with abnormally fast, slow or irregular beats);
- Shortness of breath, at rest or during physical activity;
- Fluid retention with swelling of the legs, ankles and feet;
- Tiredness;
- Sudden loss of consciousness (syncope).
Symptoms of myocarditis can resolve spontaneously, remain stable, or progressively worsen over time, until a heart transplant is required. Often, in the 2-4 weeks before presentation, patients experience flu-like signs and symptoms, such as malaise, headache, joint and muscle pain, fever, sore throat, or diarrhea. When myocarditis is more severe, it can induce: heart failure (with symptoms such as dyspnoea, fatigue, accumulation of fluid in the lungs, liver congestion, etc.) or sudden death. Patients with viral myocarditis often have concomitant pericarditis (inflammation of the membrane that lines the heart). Myocarditis is also associated with heart rhythm abnormalities including ventricular tachycardia, heart block, flutter, and atrial fibrillation.
Myocarditis in children
Symptoms of myocarditis in infants and children tend to be more nonspecific, with general malaise, loss of appetite, abdominal pain, and / or chronic cough. Additionally, pediatric patients may experience the following signs and symptoms:
- Fever;
- Respiratory difficulties;
- Rapid breathing;
- Bluish or grayish color of the skin.
Fulminant myocarditis
Fulminant myocarditis is severe inflammation of the myocardium, resulting in ventricular systolic dysfunction, cardiogenic shock, and multiorgan decompensation. In about 10% of people with myocarditis, the condition may be the causative factor in the onset of acute heart failure. If patients with fulminant myocarditis are supported adequately and in a timely manner with treatment, they can have a good recovery, with minimal long-term sequelae. Currently, the factors that determine whether or not a patient will develop fulminant myocarditis are not known, but early recognition of this disease is very important. The underlying etiology and pathogenesis of fulminant myocarditis is thought to be similar to non-fulminant inflammatory myocardial disease. Due to its rarity, however, the incidence of the condition is not well characterized.
Diagnosis
Myocarditis is due to an underlying process that causes inflammation and damage to the heart muscle, not related to some other insult. Many secondary causes, such as a heart attack (myocardial infarction), can lead to "inflammation of the myocardium, so the diagnosis of myocarditis cannot be based solely on tests that confirm the presence of the inflammatory process limited to the heart. To confirm the presence of the disease. , the doctor may proceed with an electrocardiogram (ECG), chest X-ray, echocardiogram, and blood tests. Myocardial inflammation may be suspected based on altered electrocardiographic results (T-wave inversions and ST-segment elevations) , increase in C-reactive protein and / or erythrocyte sedimentation rate (ESR) values. In patients with myocarditis, laboratory results may show: leukocytosis, eosinophilia and increased IgM (serological analysis) and cardiac troponin levels or creatinine kinase-MB (markers of myocardial damage). Definitive diagnosis requires an endomyocardial biopsy, generally ally performed in the context of an angiography, which helps to clarify the clinical-pathological correlations. A small sample of endocardial and myocardial tissue is taken and studied by an anatomopathologist in optical microscopy. The analysis of the sample, processed with immunochemical methods, allows to establish the presence of histopathological characteristics, such as "abundant edema and" infiltrate. inflammatory in the myocardial interstitium, rich in lymphocytes and macrophages. The focal destruction of myocytes explains the insufficiency of the myocardial pump.
Treatment
The prognosis and treatment of myocarditis vary according to the cause, the severity of the inflammation, the patient's age, clinical and haemodynamic data. Infections can be managed with therapy directed at the responsible pathogen (example: antibiotics for bacterial myocarditis). In the acute phase, supportive therapy, including rest, is indicated. For symptomatic patients, digoxin and some diuretic drugs promote clinical improvement.
Moderate to severe cardiac dysfunction can be supported by inotropic therapy, followed by ACE inhibitors (example: captopril, lisinopril, etc.). People who are unresponsive to conventional therapy are candidates for treatment with ventricular assist devices, high doses of vasopressors, short courses of steroids, or other drugs that reduce the immune response. Heart transplantation is reserved for very serious patients who cannot improve with conventional therapy. Long-term treatment depends on the degree of residual heart damage and the presence of heart rhythm abnormalities.
Read more: Drugs for the Treatment of Myocarditis "
Prognosis
The prognosis of myocarditis depends on the cause and the patient's general health condition. For example, in adults with simple coxsackievirus myocarditis, symptoms may begin to improve over the course of a couple of weeks. In other cases, it can take a few months to recover. If the disease is recognized early, so that adequate supportive therapy can be undertaken immediately, the long-term prognosis of patients is good.
In many people with myocarditis, damage to the heart muscle improves without therapy, and the condition-related abnormalities found on echocardiography tend to disappear. However, more severe forms can become chronic or cause permanent damage to the myocardium, which persists even after resolution of inflammation. These patients may develop dilated cardiomyopathy or progress to an advanced stage of heart failure. Heart failure with dilated left ventricle may have a good prognosis, while loss of right ventricular function, cardiac arrest and associated ventricular arrhythmias. to myocarditis are related to an unfavorable outcome.