1) Department of Internal Medicine, Athena Villa dei Pini Clinic, Piedimonte Matese (CE);
2) Division of Internal Medicine, A.G.P. Piedimonte Matese (CE);
3) Physiopathology, Diseases and Respiratory Rehabilitation Unit, AORN Monadi, Naples
In recent decades, sports culture has undergone significant changes. Competitive athletes with important ambitions, in fact, follow rigorous training schedules for the preparation, which include daily sessions of several hours and which lead to various adaptations both to the skeletal muscles, both to the cardiovascular system, and to the "respiratory system: the changes that occur on the latter" begin to be known as the "Athlete's Lung".

The respiratory system is urged to increase ventilation (VE), so much so that from a state of rest VE increases up to 25 times, from 6 l / min to 150 l / min and more. This increase in ventilation (VE) is so costly determines, in athletes, short-term effects and long-term effects.
Short-term effects
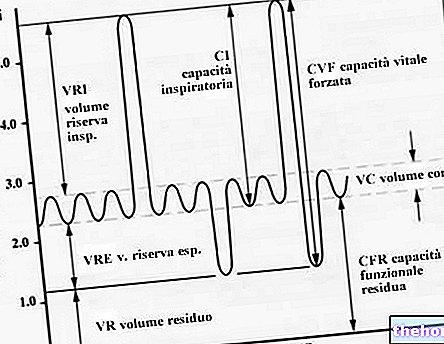
They are transient effects, in which the values of some lung parameters increase during physical exercise and / or remain higher than normal values in the following hours. An example is the residual lung volume (VR) which, conceptually analogous to functional capacity residual, measures the volume of air left in the lungs at the end of a maximal exhalation. It has been verified that its value increases following intense physical exercise, both short and long lasting (a great cycling bottom).
This value is particularly significant in the short term, according to the following table:
Measurement time
% Increase in residual lung volume
5 minutes after the end of the effort
25%
30 minutes after the end of the effort
18%
1 hour after the end of the effort
15%
This increase, however, is short-lived, as the value of the parameter returns to normal levels 24 hours after exertion.
Long-term effects
They are lasting effects, in which the values of some lung parameters increase due to physical exercise and / or remain higher than normal values in the hours that follow.
An example is the Vital Capacity (CV) which, as already underlined in the definition, measures the difference between the volume of air corresponding to the maximum inspiration and that corresponding to the maximum expiration. This lung parameter is strictly correlated to age, sex and build ( height, weight) and can be influenced by training and individual physical capabilities (performance). In fact, endurance athletes have higher vital capacity values than subjects belonging to samples of young males and females (students) (7.6 L - 8.1 L for endurance athletes, compared to lower values of 4-5 L of the control sample).
Other effects are qualitative, ie not correlated to a measurable and effective variation of the lung parameter values, as to a greater resistance to fatigue and a higher ability to maintain high dynamic parameter values for a longer period of time. In fact, part of the feeling of fatigue linked to breathing during physical activity (the "breath") is linked to the training state of the inspiratory muscles (diaphragm, intercostal, scalene). Their task is to expand the thoracic cavity, lifting the ribs and making the diaphragm descend. Since it is a muscular mechanical work, intense physical activity can cause fatigue of these muscles, which lose their effectiveness in contraction.
The purpose of training therefore does not translate into the variation of lung parameters, but into greater training of the respiratory muscles, which are able to maintain performance below the maximum ventilation values for longer intervals of time. This also means that, at the same time, the feeling of fatigue (out of breath) decreases in trained subjects. The decrease in the subjective sensation of respiratory fatigue is a phenomenon well known not only to beginner athletes, but also to opera singers, in which the only muscles used are precisely the respiratory ones (mainly the diaphragm) and who notice a notable effect of adaptation to fatigue by increasing training in the vocal and respiratory technique.
Wanting to characterize the training of the respiratory muscles with some quantitative parameters, it is necessary to consider, like any muscular work, the concentration of lactic acid in the respiratory muscles and the increase in their aerobic capacity. In particular, the training of the respiratory muscles causes a decrease in their concentration of lactic acid at the end of physical exercise, and an increase in their aerobic capacity.
To try to compensate for the muscular fatigue associated with breathing, the subjects assume a typical position that facilitates respiratory mechanics: the torso bends forward, with the trunk flexed and no longer vertical, the neck is bent forward and the mouth is open. to bring the jaw parallel to the ground. This phenomenon is often observed in long-distance running tests, for example in marathon runners or cyclists, and in many subjects with respiratory diseases that limit ventilation. In fact, it seems that this position facilitates the mechanical work of lowering the diaphragm and raising the ribs, as well as favoring the venous return to the heart.
In summary, in the "exasperation of" athletic activity we have reached today, a system, such as the respiratory system, considered untrainable until a few years ago, begins to be considered an element whose strengthening can improve performance by determining that "breath In addition, useful for achieving certain results.
.jpg)