The biliary tract forms an engineered bile transport system. This liquid, produced by the liver cells and conveyed in the biliary tract in vessels of increasing caliber, is concentrated in the gallbladder and finally poured into the small intestine to favor the digestion of dietary lipids.

From synthesis in the hepatocytes (liver cells) to the outlet in the duodenum, the bile is conveyed into vessels of gradually increasing caliber, according to the following scheme:
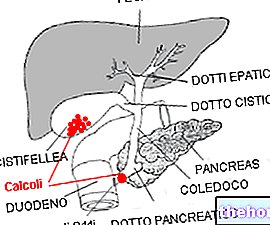
Canaliculi or biliary capillaries → Cholangioli or Hering's ductiles → Interlobular bile ducts → Intrahepatic bile ducts → Lobar hepatic ducts (right and left) that merge to form → the common hepatic duct, which exits the liver and joins with → the cystic duct (coming from the gallbladder) forming → the common bile duct (or choledochus, 7 and a half centimeters long) → which joins with the pancreatic duct → forming the ampulla of Vater → and entering the duodenum.
The common hepatic duct and the choledochus are two segments of a single canal. In fact, between meals, the bile coming from the lobar hepatic ducts enters the common hepatic duct and deviates into the gallbladder, where it is accumulated and concentrated. After a meal, when the intestine needs bile to emulsify fats and allow it to be digestion, the gallbladder (or gallbladder) contracts, pouring the accumulated bile into the duodenum. All this is favored by the presence of a sphincter, the so-called sphincter of Oddi, at the point of outlet in the small intestine; while during fasting this muscle ring is contracted, after meals it relaxes to allow the passage of bile in the intestine (contracted gallbladder -> open sphincter; relaxed gallbladder -> closed sphincter).
The outflow of bile inside the biliary tract can be obstructed at various levels by tumors, stones or strictures (abnormal narrowing). In this case we speak of cholestasis, a condition often associated with jaundice, that is, the yellow color of the skin and of the ocular sclerae due to the excessive passage of bilirubin into the circulation.
Tumors of the bile ducts
Cyst
Stenosis of the bile ducts
Stones in the common hepatic duct
Pancreatitis
Tumors of the pancreas or pseudocysts
Tumor masses in adjacent organs
Primary sclerosing cholangitis
Alcohol abuse liver disease
Amyloidosis
Bacterial abscess in the liver
Lymphoma, primary or secondary tumors of the liver
Pregnancy (obstetric cholestasis)
Primary biliary cirrhosis
Primary sclerosing cholangitis
Sarcoidosis
Sepsis
Tuberculosis
Acute viral hepatitis
Sjögren's syndrome