What is the Effluvium?
Effluvium and outflow are terms widely used in dermatology, especially in the trichological field. Evaluating whether the hair loss has the character of effluvium or outflow, acute or chronic, is in fact fundamental to frame the problems of thinning and to remedy them.

A subclassification also examines the growth phase in which the fallen hair is located.
Life cycle of the hair
In order to better understand the following classification of scents and outflows, it may be useful to open a little parenthesis on the different vital phases of the hair.
In this regard, let us briefly recall that the life cycle of a hair consists of three contiguous phases:
- Anagen phase: is the growth phase, which simultaneously affects percentages varying between 80% and 90% of the hair; its duration, of several months or even years, tends to decrease in the presence of androgenetic alopecia.
- Catagen phase: it is the phase of hair loss and lasts about two weeks.
- Telogen phase: it is the resting phase of the hair that precedes the fall (catagen), and lasts about 100 days. The length of this period tends to increase in the presence of androgenetic alopecia, up to the inversion of the temporal relationship between anagen and catagen.
We can therefore speak of effluvia in anagen, effluvia in telogen, effluvia in anagen and effluvia in telogen.
The vital phases of the hair can be evaluated by means of an examination called a trichogram.
Effluvium in Anagen

- Poisonings;
- Low-protein diet;
- Anticancer chemotherapy;
- Exposure to ionizing radiation, as occurs, for example, in the case of anticancer radiotherapy;
- Taking certain types of drugs or substances (such as, for example, cytostatic drugs, arsenic, thallium, bismuth, etc.).
Furthermore, anagen effluvium is typical of alopecia areata, which is characterized precisely by a heavy effluvium during the hair growth phase, but only in circumscribed and rounded areas.
Generally, anagen effluvium is self-limiting and lost hair will grow back spontaneously if the stressful event does not recur.
For this reason, the main treatment of anagen effluvium consists precisely in the removal of the triggering factors.
As for the treatment of alopecia areata, however, please refer to the reading of the dedicated articles already present on this site.
Effluvium in Telogen
The telogen effluvium can, in turn, be classified into telogen effluvium of the acute type and into telogen effluvium of the chronic type.
Acute telogen effluvium
Acute telogen effluvium is characterized by an intense and conspicuous hair loss (hundreds and sometimes even thousands) whose main cause is to be found in particularly stressful and short-term events and situations, such as:
- Accidents;
- Mourning;
- Childbirth;
- Surgical interventions;
- Hemorrhages;
- Febrile illnesses;
- Poisonings;
- Other acute physical or mental stress of various kinds.
However, acute telogen effluvium does not occur as a direct consequence of the above events, but approximately three months after such events.
Fortunately, the phenomenon is self-limiting and tends to resolve spontaneously within a few months. The ideal treatment for this form of effluvium, therefore, should consist only in removing the factor that caused the stress. However, in many cases, doctors still prescribe a therapy to the patient, in order to reassure him.
Regardless, the use of corticosteroids (normally employed in the chronic form) can also prove very useful in the acute form. Generally, these drugs are administered topically.
Chronic telogen effluvium

Among the main causes of chronic telogen we mention:
- Frequent blood donations;
- Severe mental illness;
- Dystyroidism;
- Chronic systemic diseases;
- Prolonged use of certain types of drugs (such as retinoids, interferon, heparin, some oral contraceptives, allopurinol, etc.);
- Nutritional deficiencies;
- Etc.
Unlike the acute form, chronic telogen effluvium does not tend to self-resolve spontaneously and the patient will face a gradual and inexorable thinning.
The treatment of chronic telogen effluvium involves intervening on the triggering cause, which can be associated with the administration of topical corticosteroids, or, in more serious cases, systemically.
Defluvium in Anagen
It is characterized by a hair loss higher than the norm, but without the dramatic characteristics of the scent. The thinning is due to the progressive loss of the follicles, secondary to their destruction. This destruction is a consequence of pathological situations that lead, in fact, to total destruction of hair follicles.
The outflow in anagen is typical of cicatricial alopecias and can occur as a result of diseases such as:
- The lichen planus;
- Discoid lupus erythematosus;
- Alopecizing folliculitis;
- Linear scleroderma (morphea);
- Broq's pseudo-area (a particular form of cicatricial alopecia);
- The trichomalacia;
- Radiation scarring alopecia.
Defluvium in Telogen
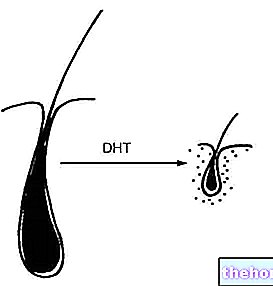
In most cases, hair loss is characterized by a telogen outflow. This is in fact the characteristic manifestation of androgenetic alopecia, a condition linked to the activity of androgens in a genetically predisposed terrain; as anticipated, this disease is characterized by moderate hair loss, accompanied by their gradual involution (they become increasingly thin, shorter and depigmented). Unlike the outflow in anagen, in androgenetic alopecia the follicle is preserved, but becomes more and more superficial.
In addition to androgenetic alopecia, both male and female, in women the defluvium in telogen is also accompanied by states of:
- Hyperprolactinemia;
- Nervous anorexia;
- Polycystic ovary syndrome;
- Androgen-secreting neoplasms;
- Hypoestrogenism (menopause, postpartum, suspension of the contraceptive pill, etc.);
- Adrenal enzyme deficiency.
The treatment of male androgenetic alopecia normally involves the administration of drugs such as finasteride and minoxidil. This last active ingredient can also be used for the treatment of female androgenetic alopecia, which can be associated with estrogen-based therapy. anyway, for more detailed information, we recommend reading the dedicated articles on this site.












.jpg)